Randomization to a Provided Higher-Complex-Carbohydrate Versus Conventional Diet in Gestational Diabetes Mellitus Results in Similar Newborn Adiposity.
Teri L Hernandez, Sarah S Farabi, Bailey K Fosdick, Nicole Hirsch, Emily Z Dunn, Kristy Rolloff, John P Corbett, Elizabeth Haugen, Tyson Marden, Janine Higgins, Jacob E Friedman, Linda A Barbour
{"title":"Randomization to a Provided Higher-Complex-Carbohydrate Versus Conventional Diet in Gestational Diabetes Mellitus Results in Similar Newborn Adiposity.","authors":"Teri L Hernandez, Sarah S Farabi, Bailey K Fosdick, Nicole Hirsch, Emily Z Dunn, Kristy Rolloff, John P Corbett, Elizabeth Haugen, Tyson Marden, Janine Higgins, Jacob E Friedman, Linda A Barbour","doi":"10.2337/dc23-0617","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Nutrition therapy for gestational diabetes mellitus (GDM) has conventionally focused on carbohydrate restriction. In a randomized controlled trial (RCT), we tested the hypothesis that a diet (all meals provided) with liberalized complex carbohydrate (60%) and lower fat (25%) (CHOICE diet) could improve maternal insulin resistance and 24-h glycemia, resulting in reduced newborn adiposity (NB%fat; powered outcome) versus a conventional lower-carbohydrate (40%) and higher-fat (45%) (LC/CONV) diet.</p><p><strong>Research design and methods: </strong>After diagnosis (at ∼28-30 weeks' gestation), 59 women with diet-controlled GDM (mean ± SEM; BMI 32 ± 1 kg/m2) were randomized to a provided LC/CONV or CHOICE diet (BMI-matched calories) through delivery. At 30-31 and 36-37 weeks of gestation, a 2-h, 75-g oral glucose tolerance test (OGTT) was performed and a continuous glucose monitor (CGM) was worn for 72 h. Cord blood samples were collected at delivery. NB%fat was measured by air displacement plethysmography (13.4 ± 0.4 days).</p><p><strong>Results: </strong>There were 23 women per group (LC/CONV [214 g/day carbohydrate] and CHOICE [316 g/day carbohydrate]). For LC/CONV and CHOICE, respectively (mean ± SEM), NB%fat (10.1 ± 1 vs. 10.5 ± 1), birth weight (3,303 ± 98 vs. 3,293 ± 81 g), and cord C-peptide levels were not different. Weight gain, physical activity, and gestational age at delivery were similar. At 36-37 weeks of gestation, CGM fasting (86 ± 3 vs. 90 ± 3 mg/dL), 1-h postprandial (119 ± 3 vs. 117 ± 3 mg/dL), 2-h postprandial (106 ± 3 vs. 108 ± 3 mg/dL), percent time in range (%TIR; 92 ± 1 vs. 91 ± 1), and 24-h glucose area under the curve values were similar between diets. The %time >120 mg/dL was statistically higher (8%) in CHOICE, as was the nocturnal glucose AUC; however, nocturnal %TIR (63-100 mg/dL) was not different. There were no between-group differences in OGTT glucose and insulin levels at 36-37 weeks of gestation.</p><p><strong>Conclusions: </strong>A ∼100 g/day difference in carbohydrate intake did not result in between-group differences in NB%fat, cord C-peptide level, maternal 24-h glycemia, %TIR, or insulin resistance indices in diet-controlled GDM.</p>","PeriodicalId":11140,"journal":{"name":"Diabetes Care","volume":" ","pages":"1931-1940"},"PeriodicalIF":14.8000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10620537/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2337/dc23-0617","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
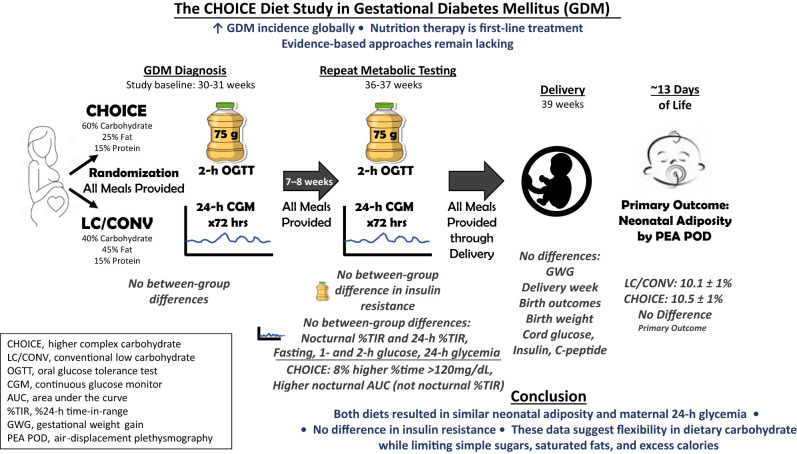
Objective: Nutrition therapy for gestational diabetes mellitus (GDM) has conventionally focused on carbohydrate restriction. In a randomized controlled trial (RCT), we tested the hypothesis that a diet (all meals provided) with liberalized complex carbohydrate (60%) and lower fat (25%) (CHOICE diet) could improve maternal insulin resistance and 24-h glycemia, resulting in reduced newborn adiposity (NB%fat; powered outcome) versus a conventional lower-carbohydrate (40%) and higher-fat (45%) (LC/CONV) diet.
Research design and methods: After diagnosis (at ∼28-30 weeks' gestation), 59 women with diet-controlled GDM (mean ± SEM; BMI 32 ± 1 kg/m2) were randomized to a provided LC/CONV or CHOICE diet (BMI-matched calories) through delivery. At 30-31 and 36-37 weeks of gestation, a 2-h, 75-g oral glucose tolerance test (OGTT) was performed and a continuous glucose monitor (CGM) was worn for 72 h. Cord blood samples were collected at delivery. NB%fat was measured by air displacement plethysmography (13.4 ± 0.4 days).
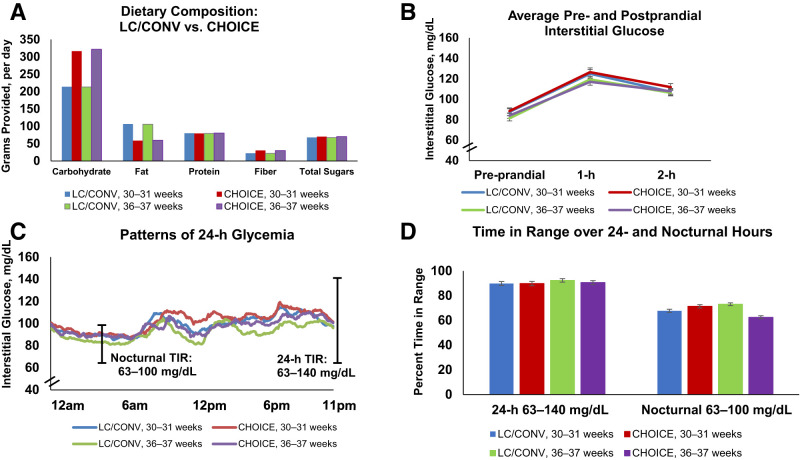
Results: There were 23 women per group (LC/CONV [214 g/day carbohydrate] and CHOICE [316 g/day carbohydrate]). For LC/CONV and CHOICE, respectively (mean ± SEM), NB%fat (10.1 ± 1 vs. 10.5 ± 1), birth weight (3,303 ± 98 vs. 3,293 ± 81 g), and cord C-peptide levels were not different. Weight gain, physical activity, and gestational age at delivery were similar. At 36-37 weeks of gestation, CGM fasting (86 ± 3 vs. 90 ± 3 mg/dL), 1-h postprandial (119 ± 3 vs. 117 ± 3 mg/dL), 2-h postprandial (106 ± 3 vs. 108 ± 3 mg/dL), percent time in range (%TIR; 92 ± 1 vs. 91 ± 1), and 24-h glucose area under the curve values were similar between diets. The %time >120 mg/dL was statistically higher (8%) in CHOICE, as was the nocturnal glucose AUC; however, nocturnal %TIR (63-100 mg/dL) was not different. There were no between-group differences in OGTT glucose and insulin levels at 36-37 weeks of gestation.
Conclusions: A ∼100 g/day difference in carbohydrate intake did not result in between-group differences in NB%fat, cord C-peptide level, maternal 24-h glycemia, %TIR, or insulin resistance indices in diet-controlled GDM.
期刊介绍:
The journal's overarching mission can be captured by the simple word "Care," reflecting its commitment to enhancing patient well-being. Diabetes Care aims to support better patient care by addressing the comprehensive needs of healthcare professionals dedicated to managing diabetes.
Diabetes Care serves as a valuable resource for healthcare practitioners, aiming to advance knowledge, foster research, and improve diabetes management. The journal publishes original research across various categories, including Clinical Care, Education, Nutrition, Psychosocial Research, Epidemiology, Health Services Research, Emerging Treatments and Technologies, Pathophysiology, Complications, and Cardiovascular and Metabolic Risk. Additionally, Diabetes Care features ADA statements, consensus reports, review articles, letters to the editor, and health/medical news, appealing to a diverse audience of physicians, researchers, psychologists, educators, and other healthcare professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


