Use of Preoperative CT Scans and Patient-Specific Instrumentation May Not Improve Short-Term Adverse Events After Shoulder Arthroplasty: Results from a Large Integrated Health-Care System.
Ronald A Navarro, Priscilla H Chan, Heather A Prentice, Michael Pearl, Frederick A Matsen Rd, Matthew D McElvany
{"title":"Use of Preoperative CT Scans and Patient-Specific Instrumentation May Not Improve Short-Term Adverse Events After Shoulder Arthroplasty: Results from a Large Integrated Health-Care System.","authors":"Ronald A Navarro, Priscilla H Chan, Heather A Prentice, Michael Pearl, Frederick A Matsen Rd, Matthew D McElvany","doi":"10.2106/JBJS.OA.22.00139","DOIUrl":null,"url":null,"abstract":"<p><p>Ongoing innovation leads to a continuous influx of new technologies related to shoulder arthroplasty. These are made available to surgeons and marketed to both health-care providers and patients with the hope of improving outcomes. We sought to evaluate how preoperative planning technologies for shoulder arthroplasty affect outcomes.</p><p><strong>Methods: </strong>This was a retrospective cohort study conducted using data from an integrated health-care system's shoulder arthroplasty registry. Adult patients who underwent primary elective anatomic or reverse total shoulder arthroplasty (2015 to 2020) were identified. Preoperative planning technologies were identified as (1) a computed tomography (CT) scan and (2) patient-specific instrumentation (PSI). Multivariable Cox regression and logistic regression were used to compare the risk of aseptic revision and 90-day adverse events, respectively, between procedures for which technologies were and were not used.</p><p><strong>Results: </strong>The study sample included 8,117 procedures (in 7,372 patients) with an average follow-up of 2.9 years (maximum, 6 years). No reduction in the risk of aseptic revision was observed for patients having either preoperative CT scans (hazard ratio [HR] = 1.22; 95% confidence interval [CI] = 0.87 to 1.72) or PSI (HR = 1.44; 95% CI = 0.71 to 2.92). Patients having CT scans had a lower likelihood of 90-day emergency department visits (odds ratio [OR] = 0.84; 95% CI = 0.73 to 0.97) but a higher likelihood of 90-day venous thromboembolic events (OR = 1.79; 95% CI = 1.18 to 2.74). Patients with PSI use had a higher likelihood of 90-day deep infection (OR = 7.74; 95% CI = 1.11 to 53.94).</p><p><strong>Conclusions: </strong>We found no reduction in the risk of aseptic revision with the use of these technologies. Patients having CT scans and PSI use had a higher likelihood of venous thromboembolism and deep infection, respectively. Ongoing research with extended follow-up is being conducted to further examine the effects of these technologies on patient outcomes.</p><p><strong>Level of evidence: </strong>Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"8 3","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2023-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1c/f0/jbjsoa-8-e22.00139.PMC10319369.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.22.00139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Ongoing innovation leads to a continuous influx of new technologies related to shoulder arthroplasty. These are made available to surgeons and marketed to both health-care providers and patients with the hope of improving outcomes. We sought to evaluate how preoperative planning technologies for shoulder arthroplasty affect outcomes.
Methods: This was a retrospective cohort study conducted using data from an integrated health-care system's shoulder arthroplasty registry. Adult patients who underwent primary elective anatomic or reverse total shoulder arthroplasty (2015 to 2020) were identified. Preoperative planning technologies were identified as (1) a computed tomography (CT) scan and (2) patient-specific instrumentation (PSI). Multivariable Cox regression and logistic regression were used to compare the risk of aseptic revision and 90-day adverse events, respectively, between procedures for which technologies were and were not used.
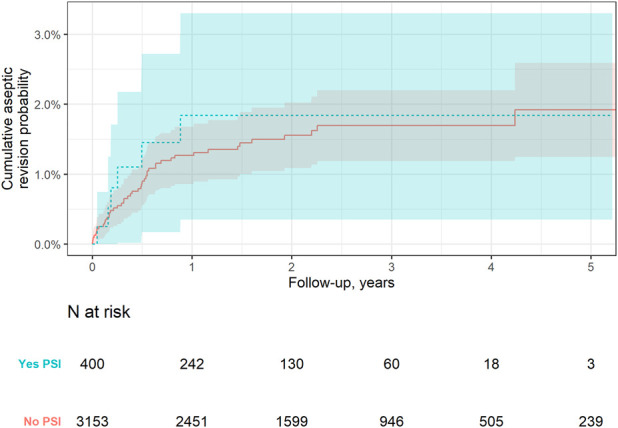
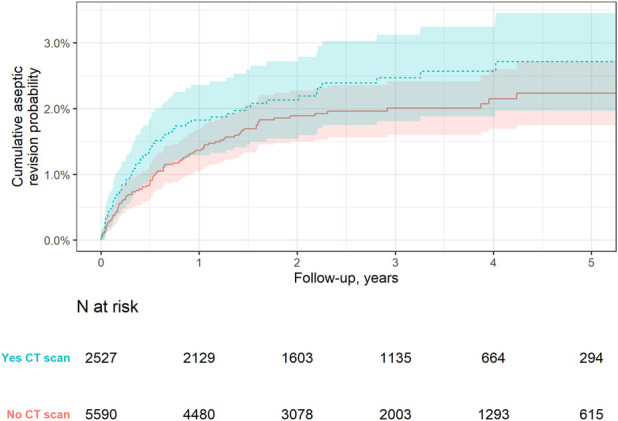
Results: The study sample included 8,117 procedures (in 7,372 patients) with an average follow-up of 2.9 years (maximum, 6 years). No reduction in the risk of aseptic revision was observed for patients having either preoperative CT scans (hazard ratio [HR] = 1.22; 95% confidence interval [CI] = 0.87 to 1.72) or PSI (HR = 1.44; 95% CI = 0.71 to 2.92). Patients having CT scans had a lower likelihood of 90-day emergency department visits (odds ratio [OR] = 0.84; 95% CI = 0.73 to 0.97) but a higher likelihood of 90-day venous thromboembolic events (OR = 1.79; 95% CI = 1.18 to 2.74). Patients with PSI use had a higher likelihood of 90-day deep infection (OR = 7.74; 95% CI = 1.11 to 53.94).
Conclusions: We found no reduction in the risk of aseptic revision with the use of these technologies. Patients having CT scans and PSI use had a higher likelihood of venous thromboembolism and deep infection, respectively. Ongoing research with extended follow-up is being conducted to further examine the effects of these technologies on patient outcomes.
Level of evidence: Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


