{"title":"Thoracic Dislocation Fracture Complicated by a Serious Electric Shock Injury: A Case Report.","authors":"Ryosuke Hirota, Atsushi Teramoto, Mitsumasa Chiba, Masahiro Onuma, Hidetomo Narimatsu, Takatoshi Yotsuyanagi, Toshihiko Yamashita","doi":"10.22603/ssrr.2023-0007","DOIUrl":null,"url":null,"abstract":"The patient, a 14-year-old boy, was injured after he collided with a high-voltage power line, which led to his loss of consciousness and caused him to fall from a 20-meterhigh steel tower. After being taken to a nearby hospital, he was flown by helicopter to our hospital for multidisciplinary treatment, where he was administered light sedation for pain relief. His initial measurements were 112/68-mmHg blood pressure, 118-beats/min heartbeat, respiratory rate of 15 breaths/ min, SpO2 of 100%, and body temperature of 38.0°C. His posterior neck, chest, and back were all severely burned (Fig. 1), and he had lost all motor and sensory function caudally from the Th10 level. He was diagnosed with an electric shock injury, a Th 10/11 dislocation fracture (AO type classification; type C), and a complete thoracic spinal cord injury. Concomitant injuries included Th 7.8.9.12 fractures, right hemothorax, left hemothorax, and multiple rib fractures (Fig. 2A-D). MRI revealed a complete spinal cord tear at the Th10/11 level (Fig. 2E). The paraspinal muscles showed high signals on MRI T2 weighted imaging, respectively (Fig. 2F-G). After confirming partial dislocation repair by manual traction under fluoroscopic guidance, we performed percutaneous posterior stabilization (Th5-L2) with percutaneous pedicle screws (PPS) without bone fusion. Relatively good realignment was achieved by intraoperative compression of the injured area in the supine position (Fig. 3A-D). On day 20 after injury, Th7-12 anterior intervertebral body fusion was performed via the extraperitoneal approach to reconstruct the anterior column (Fig. 3E-H). Debridement of burned skin was performed on the 5th, and skin grafting on the back was performed on the 35th day after the injury, respectively. The grafted skin survived well, and the wound healed completely on day 47 (Fig. 4). Rehabilitation, including wheelchair mobility training, could be started after two-stage spine surgery. On the 70th day after the injury, the wound was well-healed, and the patient was transferred to a nearby hospital. Electric shock injuries may be accompanied by deep tissue injury to the nerves, blood vessels, muscles, and bones. To our knowledge, this is the first report of severe electroshock injury combined with spinal cord injury. Recently, the concept of spine damage control has been reported in the field of spine trauma injuries, often accompanied by complications caused by high-energy trauma, such as iliac and pelvic ring fractures. Early stabilization of the spinal column promotes hemodynamic stability, respiratory failure, and systemic management and prevents complications. Initial stabilization with PPS and two-stage anterior strut reconstruction may be helpful in cases of high spinal instability and soft tissue damage. In this case, early surgery allowed good alignment without direct visual repair of the injured area. Electroshock wounds generally result in deep tissue damage, resulting in deep tissue necrosis. In particular, blood coagulation occurs after vascular injury, resulting in the progression of tissue necrosis due to hemodynamic irregularities for","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 4","pages":"410-413"},"PeriodicalIF":1.2000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e3/ab/2432-261X-7-0410.PMC10447183.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2023-0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
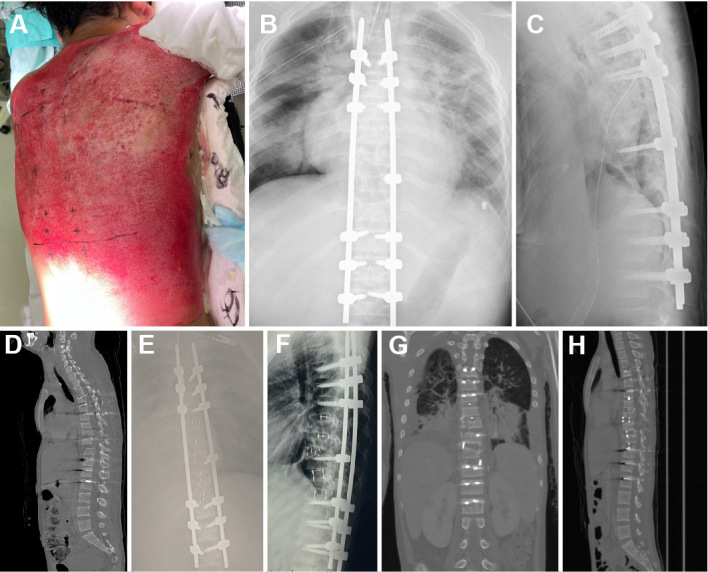
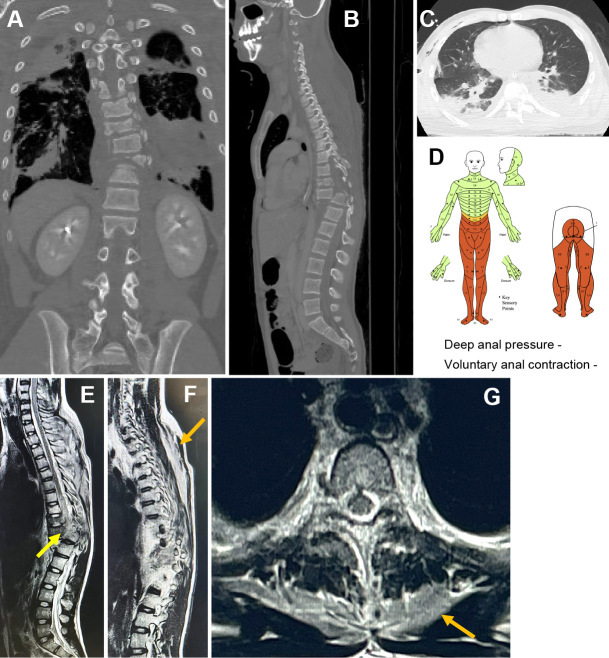
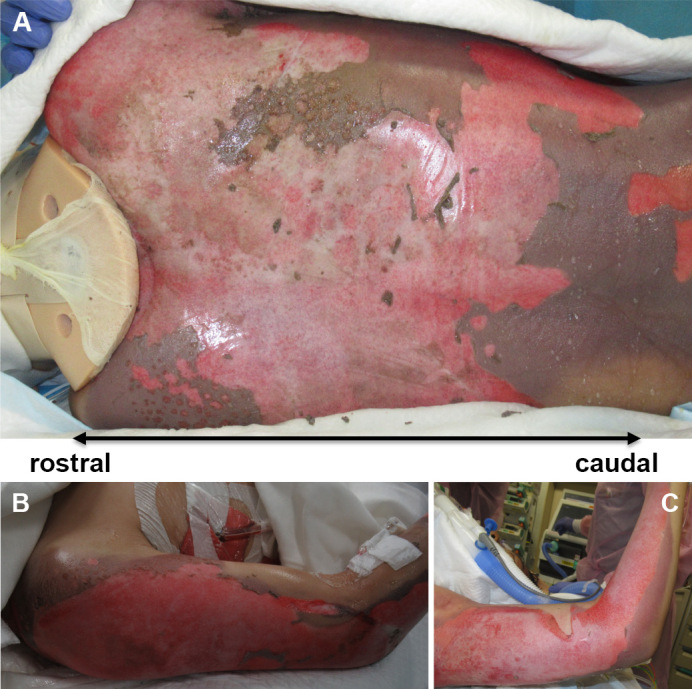
The patient, a 14-year-old boy, was injured after he collided with a high-voltage power line, which led to his loss of consciousness and caused him to fall from a 20-meterhigh steel tower. After being taken to a nearby hospital, he was flown by helicopter to our hospital for multidisciplinary treatment, where he was administered light sedation for pain relief. His initial measurements were 112/68-mmHg blood pressure, 118-beats/min heartbeat, respiratory rate of 15 breaths/ min, SpO2 of 100%, and body temperature of 38.0°C. His posterior neck, chest, and back were all severely burned (Fig. 1), and he had lost all motor and sensory function caudally from the Th10 level. He was diagnosed with an electric shock injury, a Th 10/11 dislocation fracture (AO type classification; type C), and a complete thoracic spinal cord injury. Concomitant injuries included Th 7.8.9.12 fractures, right hemothorax, left hemothorax, and multiple rib fractures (Fig. 2A-D). MRI revealed a complete spinal cord tear at the Th10/11 level (Fig. 2E). The paraspinal muscles showed high signals on MRI T2 weighted imaging, respectively (Fig. 2F-G). After confirming partial dislocation repair by manual traction under fluoroscopic guidance, we performed percutaneous posterior stabilization (Th5-L2) with percutaneous pedicle screws (PPS) without bone fusion. Relatively good realignment was achieved by intraoperative compression of the injured area in the supine position (Fig. 3A-D). On day 20 after injury, Th7-12 anterior intervertebral body fusion was performed via the extraperitoneal approach to reconstruct the anterior column (Fig. 3E-H). Debridement of burned skin was performed on the 5th, and skin grafting on the back was performed on the 35th day after the injury, respectively. The grafted skin survived well, and the wound healed completely on day 47 (Fig. 4). Rehabilitation, including wheelchair mobility training, could be started after two-stage spine surgery. On the 70th day after the injury, the wound was well-healed, and the patient was transferred to a nearby hospital. Electric shock injuries may be accompanied by deep tissue injury to the nerves, blood vessels, muscles, and bones. To our knowledge, this is the first report of severe electroshock injury combined with spinal cord injury. Recently, the concept of spine damage control has been reported in the field of spine trauma injuries, often accompanied by complications caused by high-energy trauma, such as iliac and pelvic ring fractures. Early stabilization of the spinal column promotes hemodynamic stability, respiratory failure, and systemic management and prevents complications. Initial stabilization with PPS and two-stage anterior strut reconstruction may be helpful in cases of high spinal instability and soft tissue damage. In this case, early surgery allowed good alignment without direct visual repair of the injured area. Electroshock wounds generally result in deep tissue damage, resulting in deep tissue necrosis. In particular, blood coagulation occurs after vascular injury, resulting in the progression of tissue necrosis due to hemodynamic irregularities for

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


