Akash Kartik, Catharina Müller, Miklos Acs, Pompiliu Piso, Patrick Starlinger, Thomas Bachleitner-Hofmann, Travis E Grotz
{"title":"Early postoperative CRP predicts major complications following cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC).","authors":"Akash Kartik, Catharina Müller, Miklos Acs, Pompiliu Piso, Patrick Starlinger, Thomas Bachleitner-Hofmann, Travis E Grotz","doi":"10.1515/pp-2022-0203","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Cytoreductive surgery (CRS) and heated intraperitoneal chemotherapy (HIPEC) is associated with significant postoperative complications. Early detection of at-risk patients may lead to improved outcomes. The role of C-reactive protein (CRP) in predicting postoperative complications has only been recently investigated.</p><p><strong>Methods: </strong>Postoperative complications were categorized according to Clavien-Dindo classification and further divided into minor (Grade <3) and major complications (Grade ≥3A). Absolute CRP counts (mg/L) on postoperative days (POD) 1-7, and proportional change in CRP was compared and the area under (AUC) receiver operating characteristics (ROC) curve was calculated. Univariate and multivariate analysis was performed. Significant findings were externally validated.</p><p><strong>Results: </strong>Twenty-five percent of patients experienced one or more major complications. A CRP level of ≥106 mg/L on POD 2 and 65.5 mg/L on POD 4 were significantly associated with an increased risk of major complications with an AUC of 0.658 and 0.672, respectively. The proportional increase in CRP between POD 1 and 4 (ΔCRP POD 1/4) at a cut-off of 30 % had the best AUC of 0.744 and was the only independent risk factor for major complications (p<0.0001) on multivariate analysis. ∆CRP had an AUC of 0.716 (p=0.002) when validated in an independent database.</p><p><strong>Conclusions: </strong>CRP can be used in a variety of ways to predict major complications after CRS and HIPEC. However, the ∆CRP POD 1/4>30 % is the best indicator of major complications. Serial CRP measurements in the early postoperative period may lead to early detection of patients at risk of major complications allowing for alternative management strategies to improve outcomes.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"8 3","pages":"113-121"},"PeriodicalIF":2.4000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10468822/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2022-0203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Cytoreductive surgery (CRS) and heated intraperitoneal chemotherapy (HIPEC) is associated with significant postoperative complications. Early detection of at-risk patients may lead to improved outcomes. The role of C-reactive protein (CRP) in predicting postoperative complications has only been recently investigated.
Methods: Postoperative complications were categorized according to Clavien-Dindo classification and further divided into minor (Grade <3) and major complications (Grade ≥3A). Absolute CRP counts (mg/L) on postoperative days (POD) 1-7, and proportional change in CRP was compared and the area under (AUC) receiver operating characteristics (ROC) curve was calculated. Univariate and multivariate analysis was performed. Significant findings were externally validated.
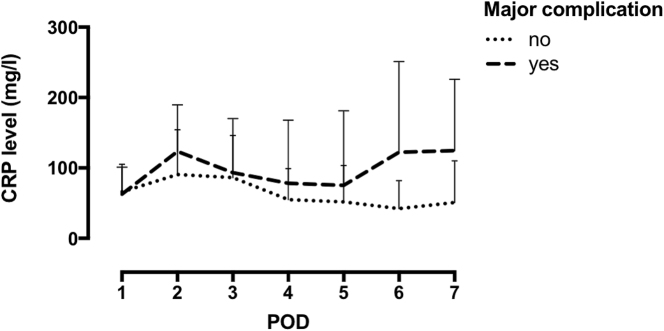
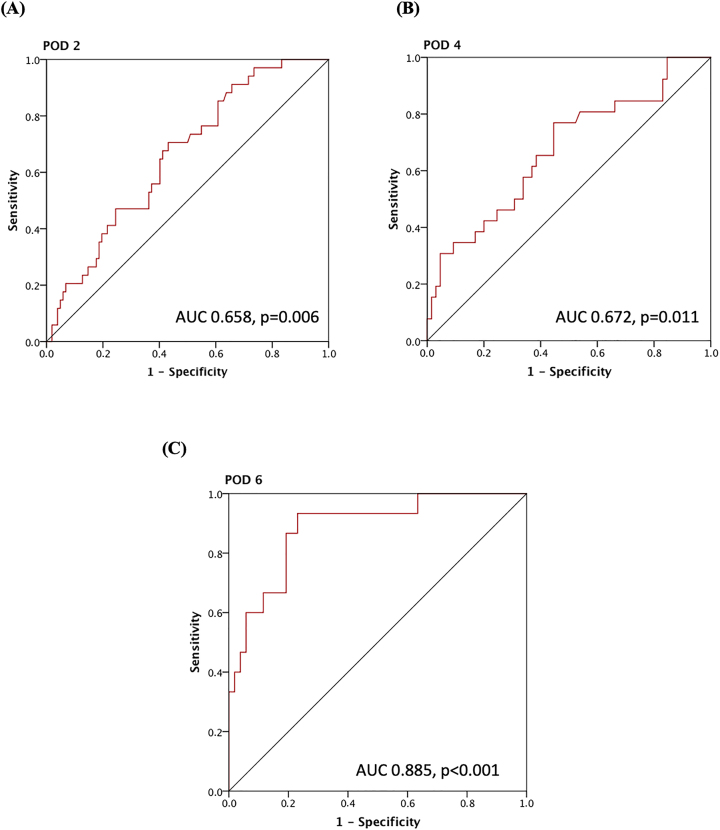
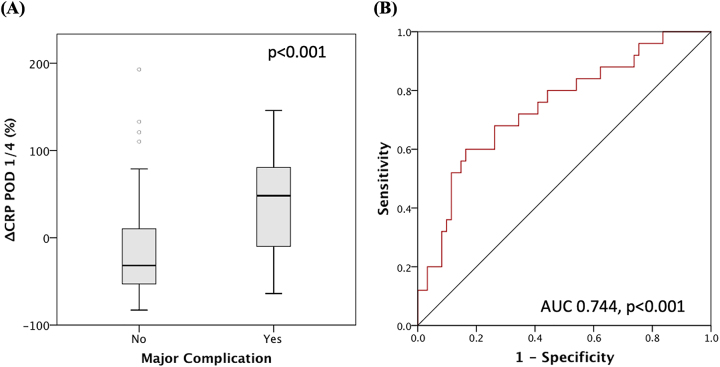
Results: Twenty-five percent of patients experienced one or more major complications. A CRP level of ≥106 mg/L on POD 2 and 65.5 mg/L on POD 4 were significantly associated with an increased risk of major complications with an AUC of 0.658 and 0.672, respectively. The proportional increase in CRP between POD 1 and 4 (ΔCRP POD 1/4) at a cut-off of 30 % had the best AUC of 0.744 and was the only independent risk factor for major complications (p<0.0001) on multivariate analysis. ∆CRP had an AUC of 0.716 (p=0.002) when validated in an independent database.
Conclusions: CRP can be used in a variety of ways to predict major complications after CRS and HIPEC. However, the ∆CRP POD 1/4>30 % is the best indicator of major complications. Serial CRP measurements in the early postoperative period may lead to early detection of patients at risk of major complications allowing for alternative management strategies to improve outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


