{"title":"Adenoid cystic carcinoma of the head and neck - treatment strategies of a highly malignant tumor with variable localizations.","authors":"Florian Dudde, Kai-Olaf Henkel, Filip Barbarewicz","doi":"10.18632/oncoscience.581","DOIUrl":null,"url":null,"abstract":"Head and neck tumors are among the most common malignancies [1]. In this anatomical region, squamous cell carcinoma (SCC) is the most common malignant entity [1]. However, there are also other malignant tumors that, unlike SCC, originate in the salivary glands of the head and neck region, such as mucoepidermoid carcinoma or adenoid cystic carcinoma (ACC) [2]. In general, tumors originating from the minor salivary glands often show a higher degree of malignancy than tumors of the major salivary glands (parotid gland, submandibular gland, sublingual gland) [2]. Consequently, the ACC in particular is often localized in the area of the hard palate (small salivary glands). In rare cases, ACC has also been described in other regions of the head and neck region, such as the paranasal sinuses or the tongue [3, 4]. The clinical features of ACC in the head and neck region are often variable. Typically, a swelling of the respective facial region that progresses quickly or slowly, depending on the growth pattern, is often associated with diffuse pain [5]. Furthermore, signs of paralysis and reduced sensitivity in the facial region are possible due to the perineural and perivascular pattern of ACC spread [5]. Most ACC usually show a slow growth pattern with a histologically highly differentiated cell picture, but markedly infiltrative growth behavior [5]. Histologically, the ACC often does not show any increased mitotic rates, which leads in particular to a lack of sensitivity towards chemotherapeutic agents [6]. In advanced ACC, even conventional radiation therapy can sometimes only achieve limited improvement with regard to the long-term outcome of ACC given the low mitotic aspect [6]. Diagnostically, three-dimensional imaging such as computed tomography and/or magnetic resonance imaging offer advantages with regard to tumor spread and the presence of metastases in the sense of tumor staging and provide important information in the context of therapy planning. Typically, ACC can show increased uptake of contrast medium agent with an infiltrative spread pattern in the respective anatomical region (Figure 1) [3].","PeriodicalId":19508,"journal":{"name":"Oncoscience","volume":"10 ","pages":"27-29"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10305238/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncoscience","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18632/oncoscience.581","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
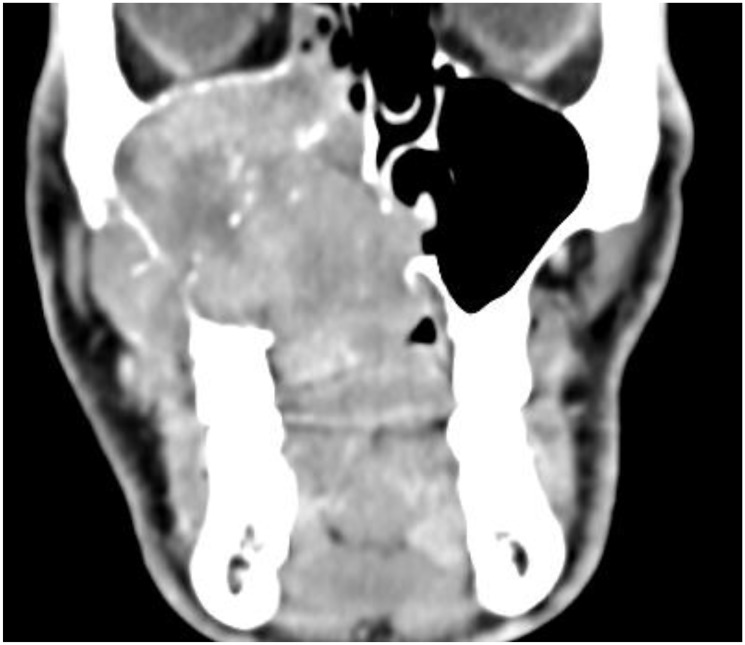
Head and neck tumors are among the most common malignancies [1]. In this anatomical region, squamous cell carcinoma (SCC) is the most common malignant entity [1]. However, there are also other malignant tumors that, unlike SCC, originate in the salivary glands of the head and neck region, such as mucoepidermoid carcinoma or adenoid cystic carcinoma (ACC) [2]. In general, tumors originating from the minor salivary glands often show a higher degree of malignancy than tumors of the major salivary glands (parotid gland, submandibular gland, sublingual gland) [2]. Consequently, the ACC in particular is often localized in the area of the hard palate (small salivary glands). In rare cases, ACC has also been described in other regions of the head and neck region, such as the paranasal sinuses or the tongue [3, 4]. The clinical features of ACC in the head and neck region are often variable. Typically, a swelling of the respective facial region that progresses quickly or slowly, depending on the growth pattern, is often associated with diffuse pain [5]. Furthermore, signs of paralysis and reduced sensitivity in the facial region are possible due to the perineural and perivascular pattern of ACC spread [5]. Most ACC usually show a slow growth pattern with a histologically highly differentiated cell picture, but markedly infiltrative growth behavior [5]. Histologically, the ACC often does not show any increased mitotic rates, which leads in particular to a lack of sensitivity towards chemotherapeutic agents [6]. In advanced ACC, even conventional radiation therapy can sometimes only achieve limited improvement with regard to the long-term outcome of ACC given the low mitotic aspect [6]. Diagnostically, three-dimensional imaging such as computed tomography and/or magnetic resonance imaging offer advantages with regard to tumor spread and the presence of metastases in the sense of tumor staging and provide important information in the context of therapy planning. Typically, ACC can show increased uptake of contrast medium agent with an infiltrative spread pattern in the respective anatomical region (Figure 1) [3].

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


