Rachel K Hechtman, Jennifer Cano, Taylor Whittington, Cainnear K Hogan, Sarah M Seelye, Jeremy B Sussman, Hallie C Prescott
{"title":"A Multi-Hospital Survey of Current Practices for Supporting Recovery From Sepsis.","authors":"Rachel K Hechtman, Jennifer Cano, Taylor Whittington, Cainnear K Hogan, Sarah M Seelye, Jeremy B Sussman, Hallie C Prescott","doi":"10.1097/CCE.0000000000000926","DOIUrl":null,"url":null,"abstract":"<p><p>Sepsis survivors are at increased risk for morbidity and functional impairment. There are recommended practices to support recovery after sepsis, but it is unclear how often they are implemented. We sought to assess the current use of recovery-based practices across hospitals.</p><p><strong>Design: </strong>Electronic survey assessing the use of best practices for recovery from COVID-related and non-COVID-related sepsis. Questions included four-point Likert responses of \"never\" to \"always/nearly always.\"</p><p><strong>Setting: </strong>Twenty-six veterans affairs hospitals with the highest (<i>n</i> = 13) and lowest (<i>n</i> = 13) risk-adjusted 90-day sepsis survival.</p><p><strong>Subjects: </strong>Inpatient and outpatient clinician leaders.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>For each domain, we calculated the proportion of \"always/nearly always\" responses and mean Likert scores. We assessed for differences by hospital survival, COVID versus non-COVID sepsis, and sepsis case volume. Across eight domains of care, the proportion \"always/nearly always\" responses ranged from: 80.7% (social support) and 69.8% (medication management) to 22.5% (physical recovery and adaptation) and 0.0% (emotional support). Higher-survival hospitals more often performed screening for new symptoms/limitations (49.2% vs 35.1% \"always/nearly always,\" <i>p</i> = 0.02) compared with lower-survival hospitals. There was no difference in \"always/nearly always\" responses for COVID-related versus non-COVID-related sepsis, but small differences in mean Likert score in four domains: care coordination (3.34 vs 3.48, <i>p</i> = 0.01), medication management (3.59 vs 3.65, <i>p</i> = 0.04), screening for new symptoms/limitations (3.13 vs 3.20, <i>p</i> = 0.02), and anticipatory guidance and education (2.97 vs 2.84, <i>p</i> < 0.001). Lower case volume hospitals more often performed care coordination (72.7% vs 43.8% \"always/nearly always,\" <i>p</i> = 0.02), screening for new symptoms/limitations (60.6% vs 35.8%, <i>p</i> < 0.001), and social support (100% vs 74.2%, <i>p</i> = 0.01).</p><p><strong>Conclusions: </strong>Our findings show variable adoption of practices for sepsis recovery. Future work is needed to understand why some practice domains are employed more frequently than others, and how to facilitate practice implementation, particularly within rarely adopted domains such as emotional support.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 6","pages":"e0926"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/12/cc9-5-e0926.PMC10456977.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000926","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Sepsis survivors are at increased risk for morbidity and functional impairment. There are recommended practices to support recovery after sepsis, but it is unclear how often they are implemented. We sought to assess the current use of recovery-based practices across hospitals.
Design: Electronic survey assessing the use of best practices for recovery from COVID-related and non-COVID-related sepsis. Questions included four-point Likert responses of "never" to "always/nearly always."
Setting: Twenty-six veterans affairs hospitals with the highest (n = 13) and lowest (n = 13) risk-adjusted 90-day sepsis survival.
Subjects: Inpatient and outpatient clinician leaders.
Interventions: None.
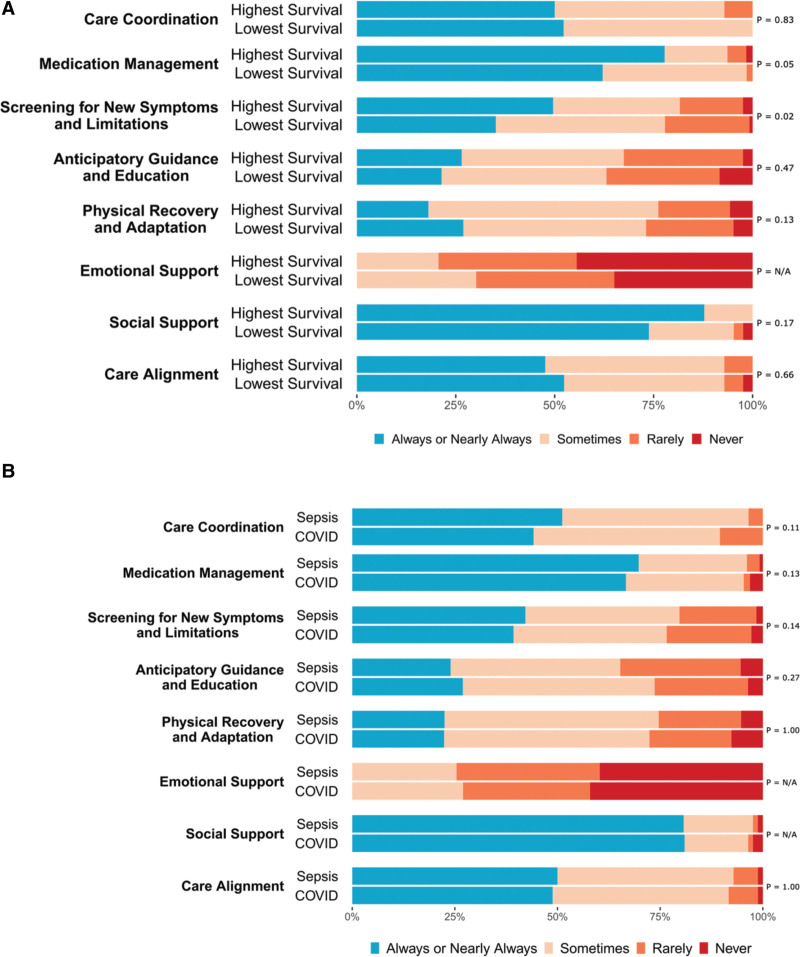
Measurements and main results: For each domain, we calculated the proportion of "always/nearly always" responses and mean Likert scores. We assessed for differences by hospital survival, COVID versus non-COVID sepsis, and sepsis case volume. Across eight domains of care, the proportion "always/nearly always" responses ranged from: 80.7% (social support) and 69.8% (medication management) to 22.5% (physical recovery and adaptation) and 0.0% (emotional support). Higher-survival hospitals more often performed screening for new symptoms/limitations (49.2% vs 35.1% "always/nearly always," p = 0.02) compared with lower-survival hospitals. There was no difference in "always/nearly always" responses for COVID-related versus non-COVID-related sepsis, but small differences in mean Likert score in four domains: care coordination (3.34 vs 3.48, p = 0.01), medication management (3.59 vs 3.65, p = 0.04), screening for new symptoms/limitations (3.13 vs 3.20, p = 0.02), and anticipatory guidance and education (2.97 vs 2.84, p < 0.001). Lower case volume hospitals more often performed care coordination (72.7% vs 43.8% "always/nearly always," p = 0.02), screening for new symptoms/limitations (60.6% vs 35.8%, p < 0.001), and social support (100% vs 74.2%, p = 0.01).
Conclusions: Our findings show variable adoption of practices for sepsis recovery. Future work is needed to understand why some practice domains are employed more frequently than others, and how to facilitate practice implementation, particularly within rarely adopted domains such as emotional support.
脓毒症幸存者的发病率和功能损害风险增加。有一些建议的做法可以支持败血症后的康复,但尚不清楚它们的实施频率。我们试图评估目前各医院使用基于康复的做法的情况。设计:电子调查,评估新冠肺炎相关和非新冠肺炎相关性败血症康复最佳实践的使用情况。问题包括Likert对“从不”到“总是/几乎总是”的四点回答。设置:26家退伍军人事务医院的败血症90天生存率最高(n=13)和最低(n=13。受试者:住院和门诊临床医生领导。干预措施:无。测量和主要结果:对于每个领域,我们计算了“总是/几乎总是”回答的比例和平均Likert分数。我们通过医院生存率、新冠肺炎与非新冠肺炎败血症以及败血症病例数来评估差异。在八个护理领域中,“总是/几乎总是”的反应比例从80.7%(社会支持)和69.8%(药物管理)到22.5%(身体恢复和适应)和0.0%(情感支持)不等。与生存率较低的医院相比,生存率较高的医院更经常进行新症状/局限性筛查(49.2%对35.1%“总是/几乎总是”,p=0.02)。与非新冠肺炎相关的败血症相比,“总是/几乎总是”的反应没有差异,但在四个领域的平均Likert评分略有差异:护理协调(3.34 vs 3.48,p=0.01)、药物管理(3.59 vs 3.65,p=0.04)、新症状/限制筛查(3.13 vs 3.20,p=0.02),以及预期指导和教育(2.97 vs 2.84,p<0.001)。病例量较低的医院更经常进行护理协调(72.7%vs 43.8%“总是/几乎总是”,p=0.02)、新症状/局限性筛查(60.6%vs 35.8%,p<001)和社会支持(100%vs 74.2%,p=0.01)。结论:我们的研究结果表明,败血症康复实践的采用情况各不相同。未来的工作需要了解为什么一些实践领域比其他领域更频繁地使用,以及如何促进实践的实施,特别是在情感支持等很少被采用的领域。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


