Meiyin Lin, Sebastian Chakrit Bhakdi, Damien Tan, Joycelyn Jie Xin Lee, David Wai Meng Tai, Andrea Pavesi, Lu-En Wai, Tina Wang, Antonio Bertoletti, Anthony Tanoto Tan
{"title":"Lytic efficiency of immunosuppressive drug-resistant armoured T cells against circulating HBV-related HCC in whole blood.","authors":"Meiyin Lin, Sebastian Chakrit Bhakdi, Damien Tan, Joycelyn Jie Xin Lee, David Wai Meng Tai, Andrea Pavesi, Lu-En Wai, Tina Wang, Antonio Bertoletti, Anthony Tanoto Tan","doi":"10.1093/immadv/ltad015","DOIUrl":null,"url":null,"abstract":"<p><p>Recurrence of hepatitis B virus-related hepatocellular carcinoma (HBV-HCC) after liver transplant (LT) is mediated by circulating tumour cells (CTCs) and exacerbated by the immunosuppressants required to prevent graft rejection. To circumvent the effects of immunosuppressants, we developed immunosuppressive drug-resistant armoured HBV-specific T-cell receptor-redirected T cells (IDRA HBV-TCR). However, their ability to eliminate HBV-HCC circulating in the whole blood has never been tested, and whether their lytic efficacy is compatible with the number of adoptively transferred T cells <i>in vivo</i> has never been measured. Hence, we developed a microscopy-based assay to quantify CTCs in whole blood. The assay was then used to quantify the efficacy of IDRA HBV-TCRs to lyse free-floating HBV-HCC cells in the presence of Tacrolimus and Mycophenolate Mofetil (MMF). We demonstrated that a panel of antibodies (AFP, GPC3, Vimentin, pan-Cytokeratin, and CD45) specific for HCC tumour antigens and immune cells can effectively differentiate HCC-CTCs in whole blood. Through dose-titration experiments, we observed that in the presence of immunosuppressive drugs, a minimum of 20 000 IDRA HBV-TCR T cells/ml of whole blood is necessary to lyse ~63.5% of free-floating HBV-HCC cells within 16 hours. In conclusion, IDRA HBV-TCR T cells can lyse free-floating HBV-HCC cells in whole blood in the presence of Tacrolimus and MMF. The quantity of IDRA-HBV TCR T cells required can be achieved by the adoptive transfer of 5 × 10<sup>6</sup> IDRA-HBV TCR-T cells/kg, supporting the utilisation of IDRA HBV-TCR T cells to eliminate CTCs as prophylaxis against recurrence after LT.</p>","PeriodicalId":73353,"journal":{"name":"Immunotherapy advances","volume":"3 1","pages":"ltad015"},"PeriodicalIF":4.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/10/ltad015.PMC10460197.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunotherapy advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/immadv/ltad015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
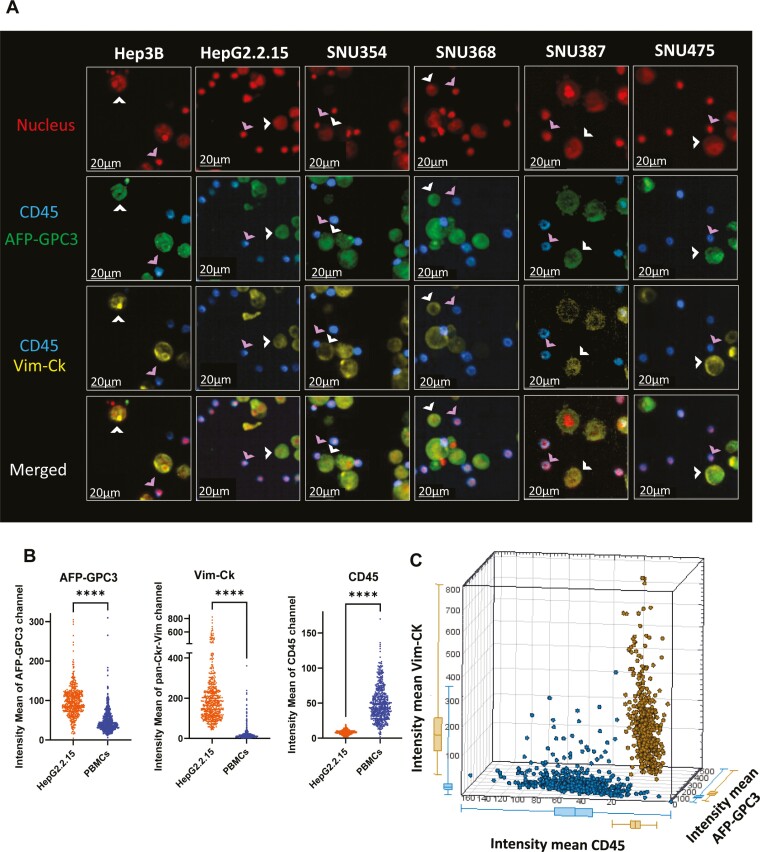
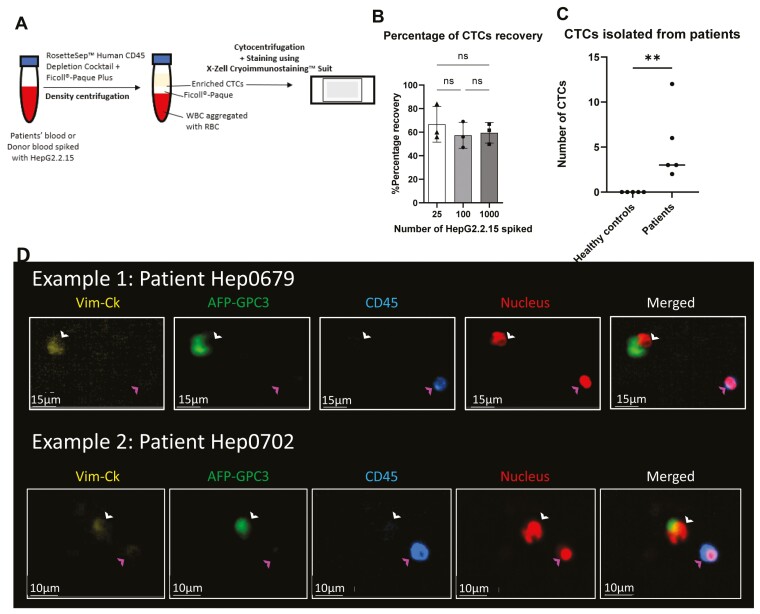
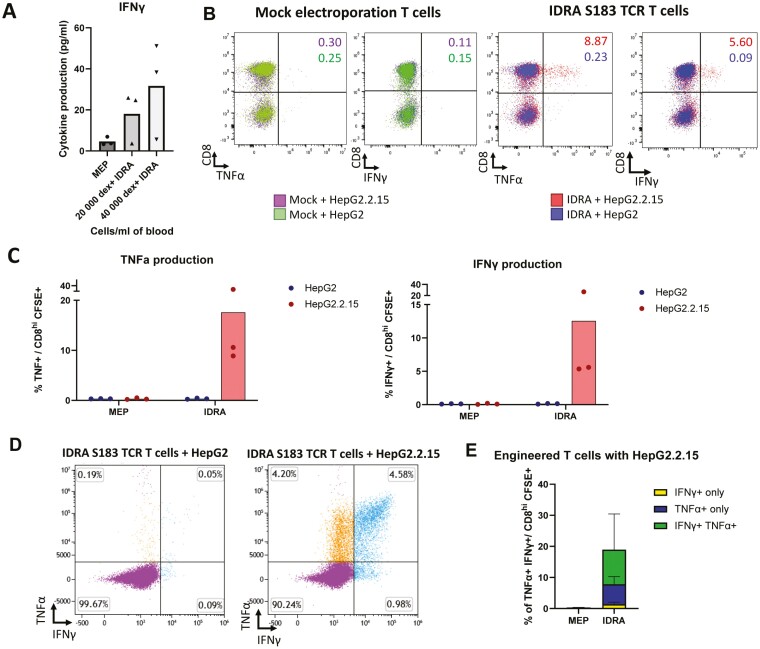
Recurrence of hepatitis B virus-related hepatocellular carcinoma (HBV-HCC) after liver transplant (LT) is mediated by circulating tumour cells (CTCs) and exacerbated by the immunosuppressants required to prevent graft rejection. To circumvent the effects of immunosuppressants, we developed immunosuppressive drug-resistant armoured HBV-specific T-cell receptor-redirected T cells (IDRA HBV-TCR). However, their ability to eliminate HBV-HCC circulating in the whole blood has never been tested, and whether their lytic efficacy is compatible with the number of adoptively transferred T cells in vivo has never been measured. Hence, we developed a microscopy-based assay to quantify CTCs in whole blood. The assay was then used to quantify the efficacy of IDRA HBV-TCRs to lyse free-floating HBV-HCC cells in the presence of Tacrolimus and Mycophenolate Mofetil (MMF). We demonstrated that a panel of antibodies (AFP, GPC3, Vimentin, pan-Cytokeratin, and CD45) specific for HCC tumour antigens and immune cells can effectively differentiate HCC-CTCs in whole blood. Through dose-titration experiments, we observed that in the presence of immunosuppressive drugs, a minimum of 20 000 IDRA HBV-TCR T cells/ml of whole blood is necessary to lyse ~63.5% of free-floating HBV-HCC cells within 16 hours. In conclusion, IDRA HBV-TCR T cells can lyse free-floating HBV-HCC cells in whole blood in the presence of Tacrolimus and MMF. The quantity of IDRA-HBV TCR T cells required can be achieved by the adoptive transfer of 5 × 106 IDRA-HBV TCR-T cells/kg, supporting the utilisation of IDRA HBV-TCR T cells to eliminate CTCs as prophylaxis against recurrence after LT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


