Ioannis Paraskevaidis, Andrew Xanthopoulos, Nikolaos Karamichalakis, Filippos Triposkiadis, Elias Tsougos
{"title":"Medical Treatment in Heart Failure with Reduced Ejection Fraction: A Proposed Algorithm Based on the Patient's Electrolytes and Congestion Status.","authors":"Ioannis Paraskevaidis, Andrew Xanthopoulos, Nikolaos Karamichalakis, Filippos Triposkiadis, Elias Tsougos","doi":"10.3390/medsci11020038","DOIUrl":null,"url":null,"abstract":"<p><p>In heart failure (HF) with reduced ejection fraction (HFrEF), four classes of drugs (β-blockers, angiotensin-converting enzyme inhibitors/angiotensin receptor neprilysin inhibitors, mineralocorticoid receptor antagonists, and the most recent Sodium-Glucose Co-Transporters 2 Inhibitors) have demonstrated positive results in randomized controlled trials (RCTs). Nevertheless, the latest RCTs are not proper for comparison since they were carried out at various times with dissimilar background therapies and the patients enrolled did not have the same characteristics. The difficulty of extrapolating from these trials and proposing a common framework appropriate for all cases is thus obvious. Despite the fact that these four agents are now the fundamental pillars of HFrEF treatment, the built-up algorithm of initiation and titration is a matter of debate. Electrolyte disturbances are common in HFrEF patients and can be attributed to several factors, such as the use of diuretics, renal impairment, and neurohormonal activation. We have identified several HFrEF phenotypes according to their sodium (Na<sup>+</sup>) and potassium (K<sup>+</sup>) status in a \"real world\" setting and suggest an algorithm on how to introduce the most appropriate drug and set up therapy based on the patients' electrolytes and the existence of congestion.</p>","PeriodicalId":74152,"journal":{"name":"Medical sciences (Basel, Switzerland)","volume":"11 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10302950/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical sciences (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medsci11020038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
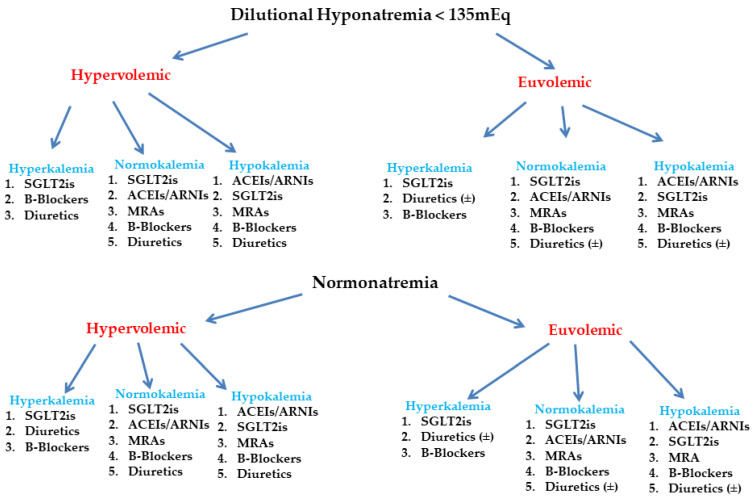
In heart failure (HF) with reduced ejection fraction (HFrEF), four classes of drugs (β-blockers, angiotensin-converting enzyme inhibitors/angiotensin receptor neprilysin inhibitors, mineralocorticoid receptor antagonists, and the most recent Sodium-Glucose Co-Transporters 2 Inhibitors) have demonstrated positive results in randomized controlled trials (RCTs). Nevertheless, the latest RCTs are not proper for comparison since they were carried out at various times with dissimilar background therapies and the patients enrolled did not have the same characteristics. The difficulty of extrapolating from these trials and proposing a common framework appropriate for all cases is thus obvious. Despite the fact that these four agents are now the fundamental pillars of HFrEF treatment, the built-up algorithm of initiation and titration is a matter of debate. Electrolyte disturbances are common in HFrEF patients and can be attributed to several factors, such as the use of diuretics, renal impairment, and neurohormonal activation. We have identified several HFrEF phenotypes according to their sodium (Na+) and potassium (K+) status in a "real world" setting and suggest an algorithm on how to introduce the most appropriate drug and set up therapy based on the patients' electrolytes and the existence of congestion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


