Amy M Cohn, Ami Sedani, Taylor Niznik, Adam Alexander, Bryce Lowery, Julia McQuoid, Janis Campbell
{"title":"Population and Neighborhood Correlates of Cannabis Dispensary Locations in Oklahoma.","authors":"Amy M Cohn, Ami Sedani, Taylor Niznik, Adam Alexander, Bryce Lowery, Julia McQuoid, Janis Campbell","doi":"10.26828/cannabis/2023.01.008","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cannabis dispensaries have proliferated exponentially in Oklahoma since the state legalized medical cannabis in 2018. Oklahoma is unique from many other legalized states given its high number of lower income, rural, and uninsured residents, who may seek medical cannabis as an alternative to traditional medical treatment.</p><p><strong>Methods: </strong>This study examined demographic and neighborhood characteristics associated with dispensary density (n = 1,046 census tracts) in Oklahoma.</p><p><strong>Results: </strong>Compared to census tracts with no dispensaries, those with at least one dispensary had a higher proportion of uninsured individuals living below the poverty level and a greater number of hospitals and pharmacies. Almost half (42.35%) of census tracts with at least one dispensary were classified as a rural locale. In fully adjusted models, percent uninsured, percent of household rentals, and the number of schools and pharmacies were positively associated with greater number of cannabis dispensaries, while the number of hospitals was negatively associated. In the best fitting interaction models, dispensaries were predominant in areas with a higher percentage of uninsured residents and no pharmacies, suggesting that cannabis retailers may capitalize on the health needs of communities with limited healthcare outlets or access to medical treatment.</p><p><strong>Conclusions: </strong>Policies and regulatory actions that seek to decrease disparities in dispensary locations should be considered. Future studies should examine whether people living in communities with a scarcity of health resources are more likely to associate cannabis with medical uses than those living in communities with more resources.</p>","PeriodicalId":72520,"journal":{"name":"Cannabis (Albuquerque, N.M.)","volume":"6 1","pages":"99-113"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/69/rsmj-6-1-99.PMC10212267.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cannabis (Albuquerque, N.M.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.26828/cannabis/2023.01.008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Cannabis dispensaries have proliferated exponentially in Oklahoma since the state legalized medical cannabis in 2018. Oklahoma is unique from many other legalized states given its high number of lower income, rural, and uninsured residents, who may seek medical cannabis as an alternative to traditional medical treatment.
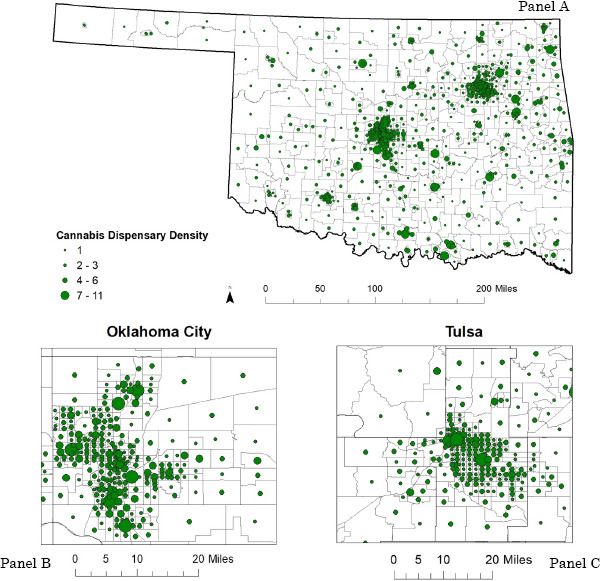
Methods: This study examined demographic and neighborhood characteristics associated with dispensary density (n = 1,046 census tracts) in Oklahoma.
Results: Compared to census tracts with no dispensaries, those with at least one dispensary had a higher proportion of uninsured individuals living below the poverty level and a greater number of hospitals and pharmacies. Almost half (42.35%) of census tracts with at least one dispensary were classified as a rural locale. In fully adjusted models, percent uninsured, percent of household rentals, and the number of schools and pharmacies were positively associated with greater number of cannabis dispensaries, while the number of hospitals was negatively associated. In the best fitting interaction models, dispensaries were predominant in areas with a higher percentage of uninsured residents and no pharmacies, suggesting that cannabis retailers may capitalize on the health needs of communities with limited healthcare outlets or access to medical treatment.
Conclusions: Policies and regulatory actions that seek to decrease disparities in dispensary locations should be considered. Future studies should examine whether people living in communities with a scarcity of health resources are more likely to associate cannabis with medical uses than those living in communities with more resources.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


