Sabine L Collette, Michael P Rodgers, Marianne A A van Walderveen, Kars C J Compagne, Paul J Nederkoorn, Jeannette Hofmeijer, Jasper M Martens, Gert J de Borst, Gert Jan R Luijckx, Charles B L M Majoie, Aad van der Lugt, Reinoud P H Bokkers, Maarten Uyttenboogaart
{"title":"Management of extracranial carotid artery stenosis during endovascular treatment for acute ischaemic stroke: results from the MR CLEAN Registry.","authors":"Sabine L Collette, Michael P Rodgers, Marianne A A van Walderveen, Kars C J Compagne, Paul J Nederkoorn, Jeannette Hofmeijer, Jasper M Martens, Gert J de Borst, Gert Jan R Luijckx, Charles B L M Majoie, Aad van der Lugt, Reinoud P H Bokkers, Maarten Uyttenboogaart","doi":"10.1136/svn-2022-001891","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal management of ipsilateral extracranial internal carotid artery (ICA) stenosis during endovascular treatment (EVT) is unclear. We compared the outcomes of two different strategies: EVT with vs without carotid artery stenting (CAS).</p><p><strong>Methods: </strong>In this observational study, we included patients who had an acute ischaemic stroke undergoing EVT and a concomitant ipsilateral extracranial ICA stenosis of ≥50% or occlusion of presumed atherosclerotic origin, from the Dutch Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry (2014-2017). The primary endpoint was a good functional outcome at 90 days, defined as a modified Rankin Scale score ≤2. Secondary endpoints were successful intracranial reperfusion, new clot in a different vascular territory, symptomatic intracranial haemorrhage, recurrent ischaemic stroke and any serious adverse event.</p><p><strong>Results: </strong>Of the 433 included patients, 169 (39%) underwent EVT with CAS. In 123/168 (73%) patients, CAS was performed before intracranial thrombectomy. In 42/224 (19%) patients who underwent EVT without CAS, a deferred carotid endarterectomy or CAS was performed. EVT with and without CAS were associated with similar proportions of good functional outcome (47% vs 42%, respectively; adjusted OR (aOR), 0.90; 95% CI, 0.50 to 1.62). There were no major differences between the groups in any of the secondary endpoints, except for the increased odds of a new clot in a different vascular territory in the EVT with CAS group (aOR, 2.96; 95% CI, 1.07 to 8.21).</p><p><strong>Conclusions: </strong>Functional outcomes were comparable after EVT with and without CAS. CAS during EVT might be a feasible option to treat the extracranial ICA stenosis but randomised studies are warranted to prove non-inferiority or superiority.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":"8 3","pages":"229-237"},"PeriodicalIF":4.9000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e3/6c/svn-2022-001891.PMC10359798.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-001891","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Background: The optimal management of ipsilateral extracranial internal carotid artery (ICA) stenosis during endovascular treatment (EVT) is unclear. We compared the outcomes of two different strategies: EVT with vs without carotid artery stenting (CAS).
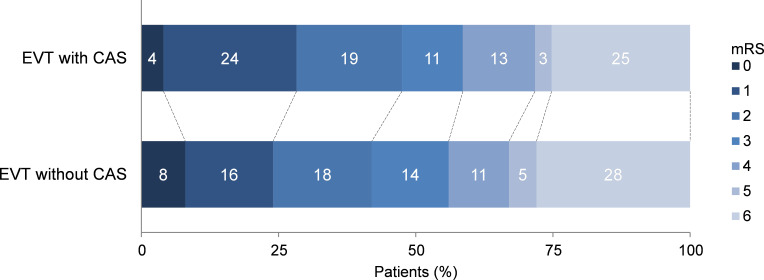
Methods: In this observational study, we included patients who had an acute ischaemic stroke undergoing EVT and a concomitant ipsilateral extracranial ICA stenosis of ≥50% or occlusion of presumed atherosclerotic origin, from the Dutch Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry (2014-2017). The primary endpoint was a good functional outcome at 90 days, defined as a modified Rankin Scale score ≤2. Secondary endpoints were successful intracranial reperfusion, new clot in a different vascular territory, symptomatic intracranial haemorrhage, recurrent ischaemic stroke and any serious adverse event.
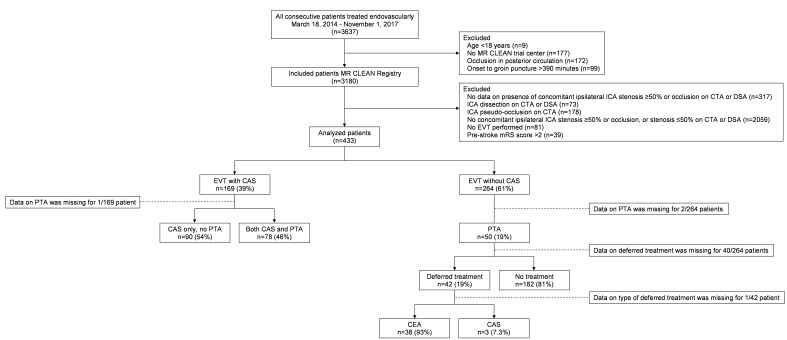
Results: Of the 433 included patients, 169 (39%) underwent EVT with CAS. In 123/168 (73%) patients, CAS was performed before intracranial thrombectomy. In 42/224 (19%) patients who underwent EVT without CAS, a deferred carotid endarterectomy or CAS was performed. EVT with and without CAS were associated with similar proportions of good functional outcome (47% vs 42%, respectively; adjusted OR (aOR), 0.90; 95% CI, 0.50 to 1.62). There were no major differences between the groups in any of the secondary endpoints, except for the increased odds of a new clot in a different vascular territory in the EVT with CAS group (aOR, 2.96; 95% CI, 1.07 to 8.21).
Conclusions: Functional outcomes were comparable after EVT with and without CAS. CAS during EVT might be a feasible option to treat the extracranial ICA stenosis but randomised studies are warranted to prove non-inferiority or superiority.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


