Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study.
Daniel R A Cox, Tess McClure, Fan Zhang, Boris Ka Leong Wong, Adam Testro, Su Kah Goh, Vijayaragavan Muralidharan, Alexander Dobrovic
{"title":"Graft-Derived Cell-Free DNA Quantification following Liver Transplantation Using Tissue-Specific DNA Methylation and Donor-Specific Genotyping Techniques: An Orthogonal Comparison Study.","authors":"Daniel R A Cox, Tess McClure, Fan Zhang, Boris Ka Leong Wong, Adam Testro, Su Kah Goh, Vijayaragavan Muralidharan, Alexander Dobrovic","doi":"10.3390/epigenomes7020011","DOIUrl":null,"url":null,"abstract":"<p><p><i>Background</i>: Graft-derived cell-free DNA (gdcfDNA) analysis has shown promise as a non-invasive tool for monitoring organ health following solid organ transplantation. A number of gdcfDNA analysis techniques have been described; however, the majority rely on sequencing or prior genotyping to detect donor-recipient mis-matched genetic polymorphisms. Differentially methylated regions of DNA can be used to identify the tissue-of-origin of cell-free DNA (cfDNA) fragments. In this study, we aimed to directly compare the performance of gdcfDNA monitoring using graft-specific DNA methylation analysis and donor-recipient genotyping techniques in a pilot cohort of clinical samples from patients post-liver transplantation. <i>Results</i>: 7 patients were recruited prior to LT, 3 developed early, biopsy-proven TCMR in the first 6 weeks post-LT. gdcfDNA was successfully quantified in all samples using both approaches. There was a high level of technical correlation between results using the two techniques (Spearman testing, r<sub>s</sub> = 0.87, <i>p</i> < 0.0001). gdcfDNA levels quantified using the genotyping approach were significantly greater across all timepoints in comparison to the tissue-specific DNA methylation-based approach: e.g., day 1 post-LT median 31,350 copies/mL (IQR 6731-64,058) vs. 4133 copies/mL (IQR 1100-8422), respectively. Qualitative trends in gdcfDNA levels for each patient were concordant between the two assays. Acute TCMR was preceded by significant elevations in gdcfDNA as quantified by both techniques. Elevations in gdcfDNA, using both techniques, were suggestive of TCMR in this pilot study with a 6- and 3-day lead-time prior to histological diagnosis in patients 1 and 2. <i>Conclusions</i>: Both the graft-specific methylation and genotyping techniques successfully quantified gdcfDNA in patients post-LT with statistically significant concordance. A direct comparison of these two techniques is not only important from a technical perspective for orthogonal validation, but significantly adds weight to the evidence that gdcfDNA monitoring reflects the underlying biology. Both techniques identified LT recipients who developed acute TCMR, with several days lead-time in comparison to conventional diagnostic workflows. Whilst the two assays performed comparably, gdcfDNA monitoring based on graft-specific DNA methylation patterns in cfDNA offers major practical advantages over the donor-recipient genotyping, and hence enhances the potential to translate this emerging technology into clinical practice.</p>","PeriodicalId":55768,"journal":{"name":"Epigenomes","volume":"7 2","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2023-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10296814/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epigenomes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/epigenomes7020011","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
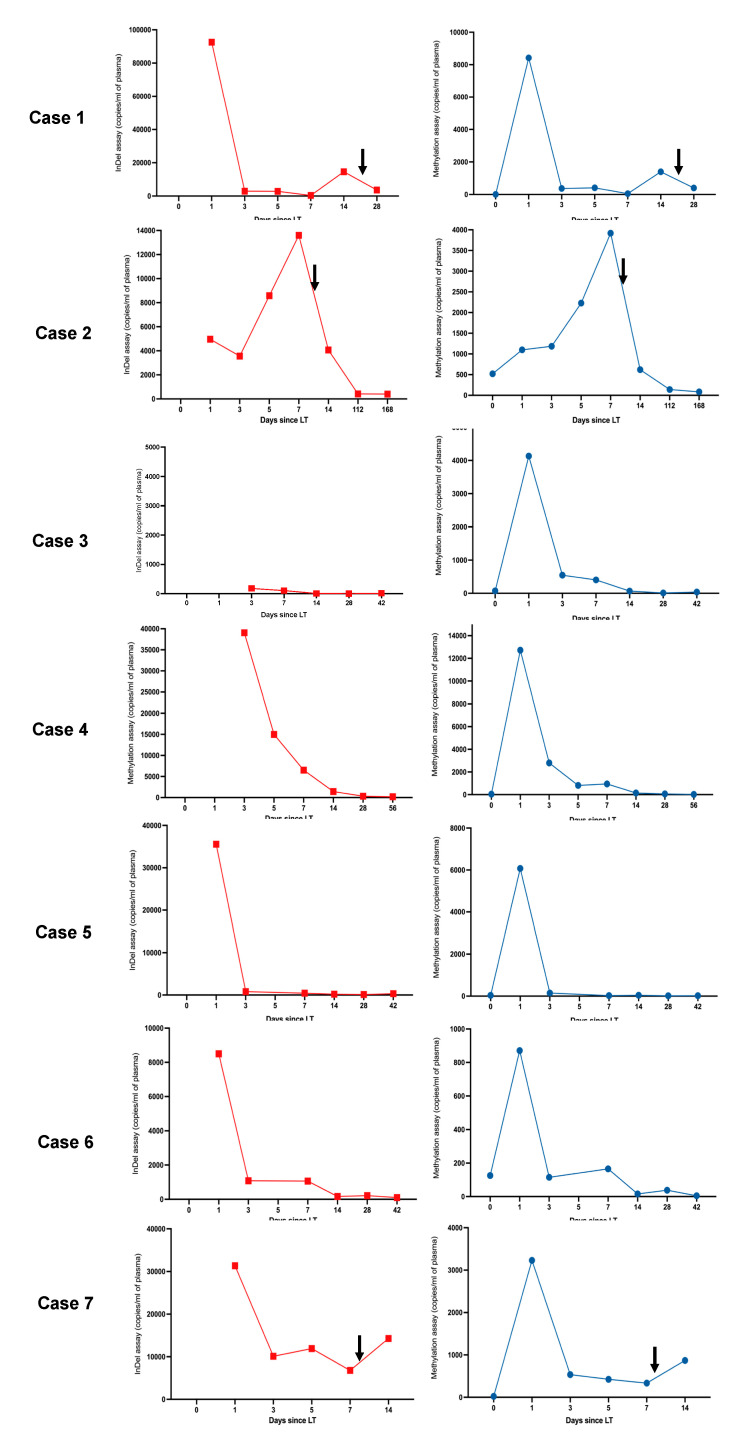
Background: Graft-derived cell-free DNA (gdcfDNA) analysis has shown promise as a non-invasive tool for monitoring organ health following solid organ transplantation. A number of gdcfDNA analysis techniques have been described; however, the majority rely on sequencing or prior genotyping to detect donor-recipient mis-matched genetic polymorphisms. Differentially methylated regions of DNA can be used to identify the tissue-of-origin of cell-free DNA (cfDNA) fragments. In this study, we aimed to directly compare the performance of gdcfDNA monitoring using graft-specific DNA methylation analysis and donor-recipient genotyping techniques in a pilot cohort of clinical samples from patients post-liver transplantation. Results: 7 patients were recruited prior to LT, 3 developed early, biopsy-proven TCMR in the first 6 weeks post-LT. gdcfDNA was successfully quantified in all samples using both approaches. There was a high level of technical correlation between results using the two techniques (Spearman testing, rs = 0.87, p < 0.0001). gdcfDNA levels quantified using the genotyping approach were significantly greater across all timepoints in comparison to the tissue-specific DNA methylation-based approach: e.g., day 1 post-LT median 31,350 copies/mL (IQR 6731-64,058) vs. 4133 copies/mL (IQR 1100-8422), respectively. Qualitative trends in gdcfDNA levels for each patient were concordant between the two assays. Acute TCMR was preceded by significant elevations in gdcfDNA as quantified by both techniques. Elevations in gdcfDNA, using both techniques, were suggestive of TCMR in this pilot study with a 6- and 3-day lead-time prior to histological diagnosis in patients 1 and 2. Conclusions: Both the graft-specific methylation and genotyping techniques successfully quantified gdcfDNA in patients post-LT with statistically significant concordance. A direct comparison of these two techniques is not only important from a technical perspective for orthogonal validation, but significantly adds weight to the evidence that gdcfDNA monitoring reflects the underlying biology. Both techniques identified LT recipients who developed acute TCMR, with several days lead-time in comparison to conventional diagnostic workflows. Whilst the two assays performed comparably, gdcfDNA monitoring based on graft-specific DNA methylation patterns in cfDNA offers major practical advantages over the donor-recipient genotyping, and hence enhances the potential to translate this emerging technology into clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


