Omar Toubat PhD , Winfield J. Wells MD , Vaughn A. Starnes MD , Subramanyan Ram Kumar MD, PhD
{"title":"Fate of the Right Ventricular Outflow Tract Following Valve-Sparing Repair of Tetralogy of Fallot","authors":"Omar Toubat PhD , Winfield J. Wells MD , Vaughn A. Starnes MD , Subramanyan Ram Kumar MD, PhD","doi":"10.1053/j.semtcvs.2022.12.002","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Valve-sparing repair (VSR) of tetralogy of Fallot<span> (TOF) tends to result in higher residual right ventricular outflow tract (RVOT) gradients. We evaluated the progression and clinical implications of RVOT gradients following VSR of TOF. Demographic, clinical, and operative data were retrospectively collected from consecutive TOF patients who underwent VSR at our institution between 01/2010 and 06/2021. RVOT gradient, </span></span>pulmonary valve annulus (PVA) diameter and Boston Z-scores were recorded from serial </span>echocardiograms<span><span>. Data are presented as median and interquartile range or number and percentage. A total of 156 children (boys 92, 59%) underwent VSR at 6.5 (4.9-8.4) months of age and 6.6 kg (5.6- 7.7) weight. There was 1 (0.6%) operative mortality. The remaining 155 patients were followed for 69.4 months (4-106.2). RVOT gradient was 2.4m/s (1.7-2.9) at discharge. It transiently increased, then declined and stabilized during follow-up. PVA Z-score was -1.7 (-3.1 to 0.5) at discharge and ‘grew’ to -0.8 (-1.7 to 0.4) at last follow-up. Freedom from RVOT re-intervention was 97%, 94% and 91% at 1, 5 and 10-year follow-up. Among 67 (43%) patients with PVA Z-score < -2, a similar RVOT gradient pattern was observed and freedom from RVOT re-intervention was 97%, 95% and 95% at 1, 5 and 8-year follow-up. Following VSR of TOF, RVOT gradients transiently increase and then fall as PVA </span>growth catches up<span>, resulting in durable intermediate outcomes. Patients with PVA Z-score < -2 demonstrated a similar pattern of hemodynamics in the RVOT and excellent freedom from reintervention.</span></span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 242-249"},"PeriodicalIF":2.6000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002817","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
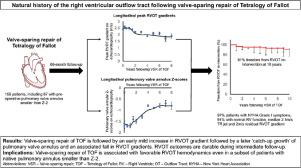
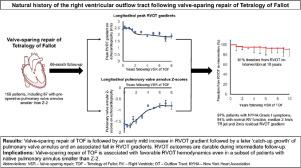
Valve-sparing repair (VSR) of tetralogy of Fallot (TOF) tends to result in higher residual right ventricular outflow tract (RVOT) gradients. We evaluated the progression and clinical implications of RVOT gradients following VSR of TOF. Demographic, clinical, and operative data were retrospectively collected from consecutive TOF patients who underwent VSR at our institution between 01/2010 and 06/2021. RVOT gradient, pulmonary valve annulus (PVA) diameter and Boston Z-scores were recorded from serial echocardiograms. Data are presented as median and interquartile range or number and percentage. A total of 156 children (boys 92, 59%) underwent VSR at 6.5 (4.9-8.4) months of age and 6.6 kg (5.6- 7.7) weight. There was 1 (0.6%) operative mortality. The remaining 155 patients were followed for 69.4 months (4-106.2). RVOT gradient was 2.4m/s (1.7-2.9) at discharge. It transiently increased, then declined and stabilized during follow-up. PVA Z-score was -1.7 (-3.1 to 0.5) at discharge and ‘grew’ to -0.8 (-1.7 to 0.4) at last follow-up. Freedom from RVOT re-intervention was 97%, 94% and 91% at 1, 5 and 10-year follow-up. Among 67 (43%) patients with PVA Z-score < -2, a similar RVOT gradient pattern was observed and freedom from RVOT re-intervention was 97%, 95% and 95% at 1, 5 and 8-year follow-up. Following VSR of TOF, RVOT gradients transiently increase and then fall as PVA growth catches up, resulting in durable intermediate outcomes. Patients with PVA Z-score < -2 demonstrated a similar pattern of hemodynamics in the RVOT and excellent freedom from reintervention.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


