C K Liu, J Milton, F-C Hsu, K M Beavers, V Yank, T Church, J D Shegog, S Kashaf, S Nayfield, A Newman, R S Stafford, B Nicklas, D E Weiner, R A Fielding
{"title":"The Effect of Chronic Kidney Disease on a Physical Activity Intervention: Impact on Physical Function, Adherence, and Safety.","authors":"C K Liu, J Milton, F-C Hsu, K M Beavers, V Yank, T Church, J D Shegog, S Kashaf, S Nayfield, A Newman, R S Stafford, B Nicklas, D E Weiner, R A Fielding","doi":"10.23937/2572-3286.1510021","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Because chronic kidney disease (CKD) is associated with muscle wasting, older adults with CKD are likely to have physical function deficits. Physical activity can improve these deficits, but whether CKD attenuates the benefits is unknown. Our objective was to determine if CKD modified the effect of a physical activity intervention in older adults.</p><p><strong>Methods: </strong>This is an exploratory analysis of the LIFE-P study, which compared a 12-month physical activity program (PA) to a successful aging education program (SA) in older adults. CKD was defined as a baseline eGFR < 60 mL/min/1.73 m<sup>2</sup>. We examined the Short Physical Performance Battery (SPPB) at baseline, 6 and 12 months. Secondary outcomes included serious adverse events (SAE) and adherence to intervention frequency. Linear mixed models were adjusted for age, sex, diabetes, hypertension, CKD, intervention, site, visit, baseline SPPB, and interactions of intervention and visit and of intervention, visit, and baseline CKD.</p><p><strong>Results: </strong>The sample included 368 participants. CKD was present in 105 (28.5%) participants with a mean eGFR of 49.2 ± 8.1 mL/min/1.73 m<sup>2</sup>. Mean SPPB was 7.38 ± 1.41 in CKD participants; 7.59 ± 1.44 in those without CKD (p = 0.20). For CKD participants in PA, 12-month SPPBs increased to 8.90 (95% CI 8.32, 9.47), while PA participants without CKD increased to 8.40 (95% CI 8.01, 8.79, p = 0.43). For CKD participants in SA, 12-month SPPBs increased to 7.67 (95% CI 7.07, 8.27), while participants without CKD increased to 8.12 (95% CI 7.72, 8.52, p = 0.86). Interaction between CKD and intervention was non-significant (p = 0.88). Number and type of SAEs were not different between CKD and non-CKD participants (all p > 0.05). In PA, adherence for CKD participants was 65.5 ± 25.4%, while for those without CKD was 74.0 ± 22.2% (p = 0.12).</p><p><strong>Conclusion: </strong>Despite lower adherence, older adults with CKD likely derive clinically meaningful benefits from physical activity with no apparent impact on safety, compared to those without CKD.</p>","PeriodicalId":73669,"journal":{"name":"Journal of clinical nephrology and renal care","volume":"3 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5937279/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical nephrology and renal care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.23937/2572-3286.1510021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/2/14 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Because chronic kidney disease (CKD) is associated with muscle wasting, older adults with CKD are likely to have physical function deficits. Physical activity can improve these deficits, but whether CKD attenuates the benefits is unknown. Our objective was to determine if CKD modified the effect of a physical activity intervention in older adults.
Methods: This is an exploratory analysis of the LIFE-P study, which compared a 12-month physical activity program (PA) to a successful aging education program (SA) in older adults. CKD was defined as a baseline eGFR < 60 mL/min/1.73 m2. We examined the Short Physical Performance Battery (SPPB) at baseline, 6 and 12 months. Secondary outcomes included serious adverse events (SAE) and adherence to intervention frequency. Linear mixed models were adjusted for age, sex, diabetes, hypertension, CKD, intervention, site, visit, baseline SPPB, and interactions of intervention and visit and of intervention, visit, and baseline CKD.
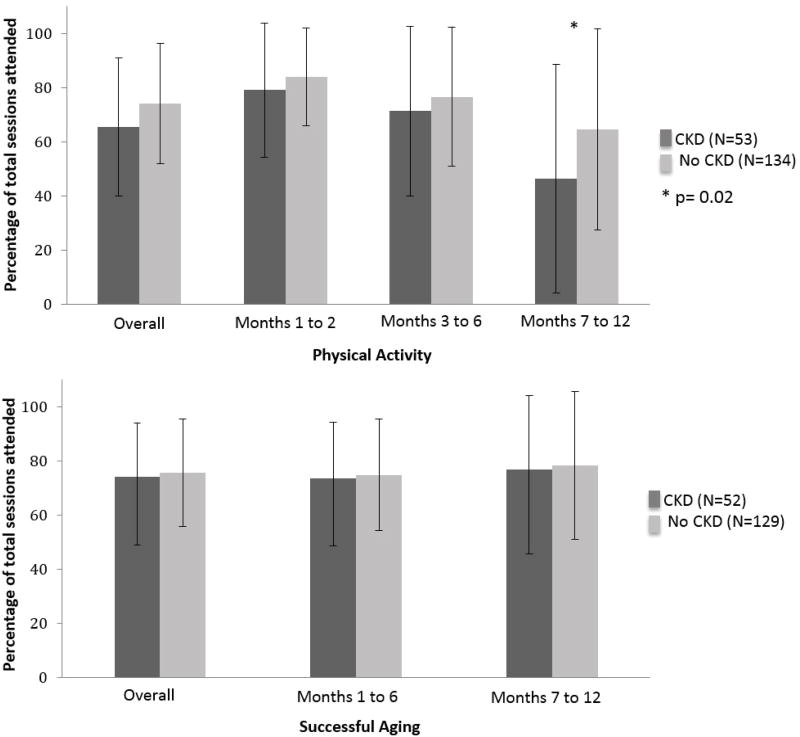
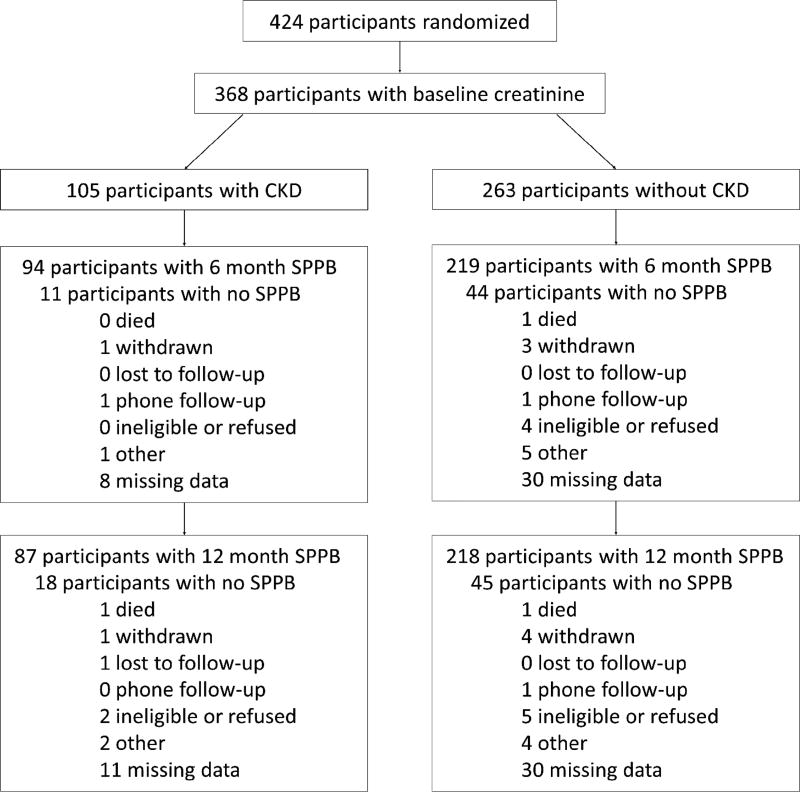
Results: The sample included 368 participants. CKD was present in 105 (28.5%) participants with a mean eGFR of 49.2 ± 8.1 mL/min/1.73 m2. Mean SPPB was 7.38 ± 1.41 in CKD participants; 7.59 ± 1.44 in those without CKD (p = 0.20). For CKD participants in PA, 12-month SPPBs increased to 8.90 (95% CI 8.32, 9.47), while PA participants without CKD increased to 8.40 (95% CI 8.01, 8.79, p = 0.43). For CKD participants in SA, 12-month SPPBs increased to 7.67 (95% CI 7.07, 8.27), while participants without CKD increased to 8.12 (95% CI 7.72, 8.52, p = 0.86). Interaction between CKD and intervention was non-significant (p = 0.88). Number and type of SAEs were not different between CKD and non-CKD participants (all p > 0.05). In PA, adherence for CKD participants was 65.5 ± 25.4%, while for those without CKD was 74.0 ± 22.2% (p = 0.12).
Conclusion: Despite lower adherence, older adults with CKD likely derive clinically meaningful benefits from physical activity with no apparent impact on safety, compared to those without CKD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


