Socio-economic, education, and insurance-related factors associated with the treatment completion rates in patients with nonmetastatic urinary bladder cancer: A Retrospective cohort study.
{"title":"Socio-economic, education, and insurance-related factors associated with the treatment completion rates in patients with nonmetastatic urinary bladder cancer: A Retrospective cohort study.","authors":"Gorrepati Rohith, Abhay Singh Gaur, Prasant Nayak, Swarnendu Mandal, Manoj K Das, Santosh Kumaraswamy, Vivek Tarigopula, Sambit Tripathy","doi":"10.4103/iju.iju_116_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Among urological malignancies, the diagnosis and treatment of urinary bladder cancer (UBC) incurs the highest cost per patient. Our objective was to broaden the current understanding of how demographic, socioeconomic, education, and insurance-related factors influence UBC management.</p><p><strong>Methods: </strong>Between January 2017 and December 2019, all patients with nonmetastatic bladder cancer were included. The demographic, treatment, and follow-up details were retrieved from a prospectively maintained database, and the Modified Kuppuswamy Index was used to evaluate the patients' socioeconomic level. Patients were divided into the completed treatment group, or the incomplete treatment group based on adherence to the initially intended treatment plan. Patients who presented with benign disease or metastases were not included.</p><p><strong>Results: </strong>Eighty-nine patients did not complete the initially intended course of treatment out of 132 patients who needed additional management after the initial transurethral resection. Comparable risk factors and demographic profiles existed in both groups. Patients with intermediate-risk disease are more likely to fail to adhere to the initial intended treatment (odds ratio [OR] = 0.09; 95% confidence interval [CI]: 0.02-0.30). On logistic regression analysis, upper socioeconomic status (OR = 6.8; 95% CI: 0.35-132.1) patients and patients with higher educational status of graduation or above (OR = 3.62; 95% CI: 0.75-17.43) had higher chances of treatment completion. Education status significantly impacted treatment completion on multivariate analysis (<i>P</i> = 0.01). Patients who utilized employer-funded insurance had better treatment compliance (OR = 4.1; 95% CI: 0.90-18.7). The compliance was unaffected by smoking, occupation, or other demographic factors.</p><p><strong>Conclusion: </strong>Patients with low economic status, low levels of education, and who need adjuvant intravesical therapy had considerably greater treatment dropout rates.</p>","PeriodicalId":47352,"journal":{"name":"Indian Journal of Urology","volume":"39 3","pages":"228-235"},"PeriodicalIF":0.9000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/c7/IJU-39-228.PMC10419770.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/iju.iju_116_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Among urological malignancies, the diagnosis and treatment of urinary bladder cancer (UBC) incurs the highest cost per patient. Our objective was to broaden the current understanding of how demographic, socioeconomic, education, and insurance-related factors influence UBC management.
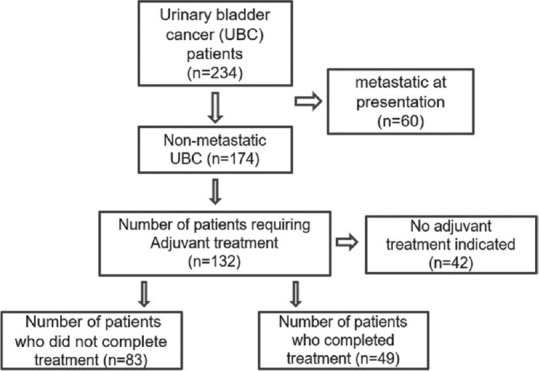
Methods: Between January 2017 and December 2019, all patients with nonmetastatic bladder cancer were included. The demographic, treatment, and follow-up details were retrieved from a prospectively maintained database, and the Modified Kuppuswamy Index was used to evaluate the patients' socioeconomic level. Patients were divided into the completed treatment group, or the incomplete treatment group based on adherence to the initially intended treatment plan. Patients who presented with benign disease or metastases were not included.
Results: Eighty-nine patients did not complete the initially intended course of treatment out of 132 patients who needed additional management after the initial transurethral resection. Comparable risk factors and demographic profiles existed in both groups. Patients with intermediate-risk disease are more likely to fail to adhere to the initial intended treatment (odds ratio [OR] = 0.09; 95% confidence interval [CI]: 0.02-0.30). On logistic regression analysis, upper socioeconomic status (OR = 6.8; 95% CI: 0.35-132.1) patients and patients with higher educational status of graduation or above (OR = 3.62; 95% CI: 0.75-17.43) had higher chances of treatment completion. Education status significantly impacted treatment completion on multivariate analysis (P = 0.01). Patients who utilized employer-funded insurance had better treatment compliance (OR = 4.1; 95% CI: 0.90-18.7). The compliance was unaffected by smoking, occupation, or other demographic factors.
Conclusion: Patients with low economic status, low levels of education, and who need adjuvant intravesical therapy had considerably greater treatment dropout rates.
期刊介绍:
Indian Journal of Urology-IJU (ISSN 0970-1591) is official publication of the Urological Society of India. The journal is published Quarterly. Bibliographic listings: The journal is indexed with Abstracts on Hygiene and Communicable Diseases, CAB Abstracts, Caspur, DOAJ, EBSCO Publishing’s Electronic Databases, Excerpta Medica / EMBASE, Expanded Academic ASAP, Genamics JournalSeek, Global Health, Google Scholar, Health & Wellness Research Center, Health Reference Center Academic, Hinari, Index Copernicus, IndMed, OpenJGate, PubMed, Pubmed Central, Scimago Journal Ranking, SCOLOAR, SCOPUS, SIIC databases, SNEMB, Tropical Diseases Bulletin, Ulrich’s International Periodical Directory

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


