{"title":"Primary Arthroplasty for Unstable and Failed Intertrochanteric Fractures: Role of Multi-Planar Trochanteric Wiring Technique.","authors":"Javahir A Pachore, Vikram Indrajit Shah, Sachin Upadhyay, Shrikunj Babulal Patel","doi":"10.5371/hp.2023.35.2.108","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The primary objective of the current study is to demonstrate the trochanteric wiring technique. A secondary objective is to evaluate the clinico-radiological outcomes of use of the wiring technique during primary arthroplasty for treatment of unstable and failed intertrochanteric fractures.</p><p><strong>Materials and methods: </strong>A prospective study including follow-up of 127 patients with unstable and failed intertrochanteric fractures who underwent primary hip arthroplasty using novel multi-planar trochanteric wiring was conducted. The average follow-up period was 17.8±4.7 months. Clinical assessment was performed using the Harris hip score (HHS). Radiographic evaluation was performed for assessment of union of the trochanter and any mechanical failure. <i>P</i><0.05 was considered statistically significant.</p><p><strong>Results: </strong>At the latest follow-up, the mean HHS showed significant improvement from 79.9±1.8 (at three months) to 91.6±5.1 (<i>P</i><0.05). In addition, no significant difference in the HHS was observed between male and female patients (<i>P</i>=0.29) and between fresh and failed intertrochanteric fractures (<i>P</i>=0.08). Union was achieved in all cases of fractured trochanter, except one. Wire breakage was observed in three patients. There were five cases of limb length discrepancy, three cases of lurch, and three cases of wire-related bursitis. There were no cases of dislocation or infection. Radiographs showed stable prosthesis in situ with no evidence of subsidence.</p><p><strong>Conclusion: </strong>Use of the proposed wiring technique was helpful in restoring the abductor level arm and multi-planar stability, which enabled better rehabilitation and resulted in excellent clinical and radiological outcomes with minimal risk of mechanical failure.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"35 2","pages":"108-121"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/15/hp-35-108.PMC10264227.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2023.35.2.108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
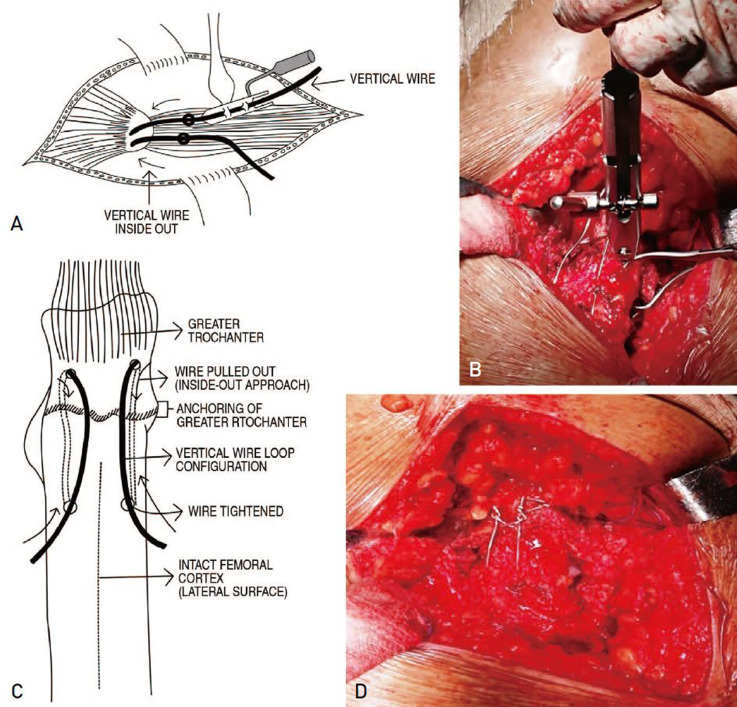
Purpose: The primary objective of the current study is to demonstrate the trochanteric wiring technique. A secondary objective is to evaluate the clinico-radiological outcomes of use of the wiring technique during primary arthroplasty for treatment of unstable and failed intertrochanteric fractures.
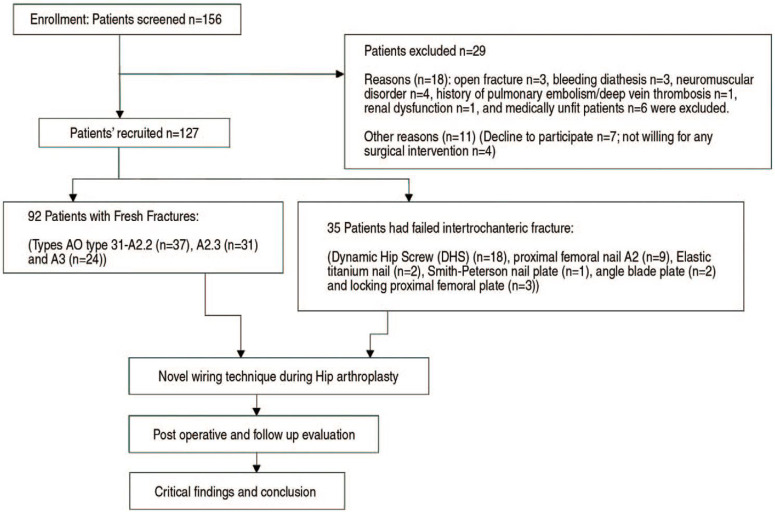
Materials and methods: A prospective study including follow-up of 127 patients with unstable and failed intertrochanteric fractures who underwent primary hip arthroplasty using novel multi-planar trochanteric wiring was conducted. The average follow-up period was 17.8±4.7 months. Clinical assessment was performed using the Harris hip score (HHS). Radiographic evaluation was performed for assessment of union of the trochanter and any mechanical failure. P<0.05 was considered statistically significant.
Results: At the latest follow-up, the mean HHS showed significant improvement from 79.9±1.8 (at three months) to 91.6±5.1 (P<0.05). In addition, no significant difference in the HHS was observed between male and female patients (P=0.29) and between fresh and failed intertrochanteric fractures (P=0.08). Union was achieved in all cases of fractured trochanter, except one. Wire breakage was observed in three patients. There were five cases of limb length discrepancy, three cases of lurch, and three cases of wire-related bursitis. There were no cases of dislocation or infection. Radiographs showed stable prosthesis in situ with no evidence of subsidence.
Conclusion: Use of the proposed wiring technique was helpful in restoring the abductor level arm and multi-planar stability, which enabled better rehabilitation and resulted in excellent clinical and radiological outcomes with minimal risk of mechanical failure.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


