Hyeong Ju Byeon, JaeSang Ko, Jun Yong Kim, Jin Sook Yoon
{"title":"Kimura Disease with Lacrimal Sac and Nasolacrimal Duct Involvement: A Case Report.","authors":"Hyeong Ju Byeon, JaeSang Ko, Jun Yong Kim, Jin Sook Yoon","doi":"10.3341/kjo.2023.0013","DOIUrl":null,"url":null,"abstract":"Dear Editor, Kimura disease (KD) is a rare allergic or autoimmune chronic inflammatory disease of the soft tissue in the head and neck region. Painless subcutaneous masses are presented in the salivary glands, lymph nodes, or deep subcutaneous tissue, which frequently occur in young Asian men. The periocular invasion has been reported in orbit, lacrimal gland, and medial canthus [1,2]. However, the invasion of the nasolacrimal duct along the inside of the lacrimal sac has not been reported. Compared to the angiolymphoid hyperplasia with eosinophilia (ALHE), KD extends to deeper tissue, and when the lacrimal sac or nasolacrimal duct is invaded, epiphora can be the main symptom. Furthermore, in a fibroinf lammatory disease spectrum, immunoglobulin G4-related disease (IgG4-RD) should be differentially diagnosed. Herein, we report a case of KD with lacrimal sac and nasolacrimal duct involvement, along with the differential diagnosis process. Informed consent for publication of the research details and clinical photographs was obtained from the patient. A 64-year-old man presented with enlarged swelling of both his inner canthus accompanied by bilateral tearing for ten months (Fig. 1A). He had no history of surgery or trauma at the periorbital area and only had a medical history of hypertension and hypertensive chronic renal failure. On physical examination, a hard palpable mass at the medial canthus and tear trough area was noted in both eyes, and the lymph nodes behind the ear were palpated. Orbital magnetic resonance image revealed T1-weighted contrast-enhanced soft tissues not only in both medial canthi but also in the lacrimal sac and along nasolacrimal ducts (Fig. 1C, 1D). He underwent an incisional biopsy on the mass at his left medial canthus. In histopathological examination, lymphoid follicles with germinal centers and eosinophilic abscess were formed in the stromal fibrosis, and abundant eosinophils and IgG4 plasma cells were infiltrated (Fig. 1E–1H). Blood samples showed eosinophilia (15.6%; normal range, 0%–7%), elevation in serum IgE level (>5,000 IU/mL; normal range, 0–100 IU/mL), and normal range of serum IgG quantitation (1,253 mg/dL; normal range, 700–1,600 mg/dL) and IgG4 concentrations (1,120 mg/L; normal range, 30–2,010 mg/L). Based on the patient’s clinical features, histological examination, and blood tests, the patient was diagnosed with KD. After the patient was administered 30 mg of prednisolone for a week, the symptoms improved (Fig. 1B), and the steroid was tapered out. The patient in the present report had KD invasion in the lacrimal sac and nasolacrimal duct as well as medial canthus, causing epiphora and palpable masses. For a differential diagnosis with ALHE and IgG4-RD, the location of occurrence, clinical features, histopathology, and serology should be comprehensively considered. Unlike ALHE, which is a benign vascular proliferative tumor manifested as more superficial hemangiomatous papules or nodules on Received: February 8, 2023 Final revision: April 14, 2023 Accepted: May 15, 2023","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":"37 3","pages":"281-283"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/75/c2/kjo-2023-0013.PMC10270775.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2023.0013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
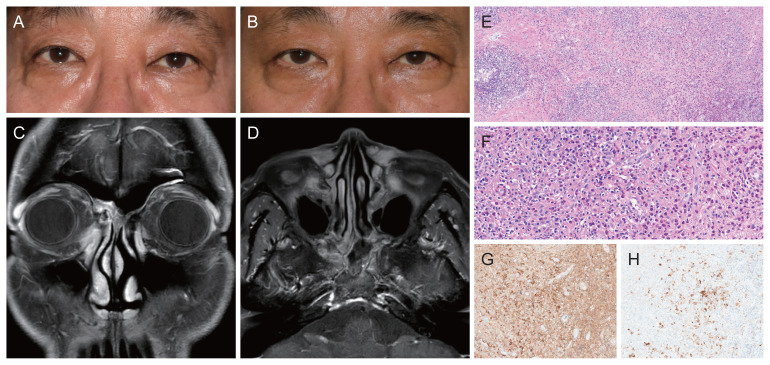
Dear Editor, Kimura disease (KD) is a rare allergic or autoimmune chronic inflammatory disease of the soft tissue in the head and neck region. Painless subcutaneous masses are presented in the salivary glands, lymph nodes, or deep subcutaneous tissue, which frequently occur in young Asian men. The periocular invasion has been reported in orbit, lacrimal gland, and medial canthus [1,2]. However, the invasion of the nasolacrimal duct along the inside of the lacrimal sac has not been reported. Compared to the angiolymphoid hyperplasia with eosinophilia (ALHE), KD extends to deeper tissue, and when the lacrimal sac or nasolacrimal duct is invaded, epiphora can be the main symptom. Furthermore, in a fibroinf lammatory disease spectrum, immunoglobulin G4-related disease (IgG4-RD) should be differentially diagnosed. Herein, we report a case of KD with lacrimal sac and nasolacrimal duct involvement, along with the differential diagnosis process. Informed consent for publication of the research details and clinical photographs was obtained from the patient. A 64-year-old man presented with enlarged swelling of both his inner canthus accompanied by bilateral tearing for ten months (Fig. 1A). He had no history of surgery or trauma at the periorbital area and only had a medical history of hypertension and hypertensive chronic renal failure. On physical examination, a hard palpable mass at the medial canthus and tear trough area was noted in both eyes, and the lymph nodes behind the ear were palpated. Orbital magnetic resonance image revealed T1-weighted contrast-enhanced soft tissues not only in both medial canthi but also in the lacrimal sac and along nasolacrimal ducts (Fig. 1C, 1D). He underwent an incisional biopsy on the mass at his left medial canthus. In histopathological examination, lymphoid follicles with germinal centers and eosinophilic abscess were formed in the stromal fibrosis, and abundant eosinophils and IgG4 plasma cells were infiltrated (Fig. 1E–1H). Blood samples showed eosinophilia (15.6%; normal range, 0%–7%), elevation in serum IgE level (>5,000 IU/mL; normal range, 0–100 IU/mL), and normal range of serum IgG quantitation (1,253 mg/dL; normal range, 700–1,600 mg/dL) and IgG4 concentrations (1,120 mg/L; normal range, 30–2,010 mg/L). Based on the patient’s clinical features, histological examination, and blood tests, the patient was diagnosed with KD. After the patient was administered 30 mg of prednisolone for a week, the symptoms improved (Fig. 1B), and the steroid was tapered out. The patient in the present report had KD invasion in the lacrimal sac and nasolacrimal duct as well as medial canthus, causing epiphora and palpable masses. For a differential diagnosis with ALHE and IgG4-RD, the location of occurrence, clinical features, histopathology, and serology should be comprehensively considered. Unlike ALHE, which is a benign vascular proliferative tumor manifested as more superficial hemangiomatous papules or nodules on Received: February 8, 2023 Final revision: April 14, 2023 Accepted: May 15, 2023

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



