Vishnupriya Khatri, Maryrose Bauschka, Meghan Foley, Cheryl Lundberg, Philip Mehler
{"title":"多学科方法治疗神经性厌食症终末期肾脏疾病1例报告。","authors":"Vishnupriya Khatri, Maryrose Bauschka, Meghan Foley, Cheryl Lundberg, Philip Mehler","doi":"10.1177/11795476231169385","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Renal dysfunction and electrolyte abnormalities are common complications of anorexia nervosa (AN), particularly in the binge-eating/purging type (AN-BP). Hypokalemic, or kaliopenic, nephropathy is an established clinical entity and a leading cause of end-stage renal disease (ESRD) in AN. Here, we present a case which demonstrates the difficulties of managing refeeding and nutrition in a psychiatrically and medically complex patient with severe AN-BP and ESRD most likely secondary to hypokalemic nephropathy.</p><p><strong>Case report: </strong>A 54-year-old female with AN-BP that has resulted in chronic hypokalemia, with newly diagnosed ESRD on hemodialysis, presented to an eating disorder medical stabilization unit for weight restoration and treatment of the medical complications associated with her severe malnutrition and ESRD. She was admitted with a body mass index (BMI) of 15 kg/m<sup>2</sup>, serum potassium of 2.8 mmol/L and serum creatinine of 6.91 mg/dL. She had failed to gain weight in the outpatient setting while on hemodialysis. She initially denied having an eating disorder, but ultimately a history of excessive laxative abuse for many years, without primary physician follow up, was revealed. While she did not undergo a renal biopsy to confirm the etiology of her ESRD, given her history of long-standing hypokalemia and lack of other risk factors, her ESRD was presumed to be secondary to hypokalemic nephropathy. She required significant oversight from a multidisciplinary eating disorder treatment team to restore weight while also managing her ESRD.</p><p><strong>Conclusion: </strong>This case report highlights the complexity of managing ESRD in patients with AN who require weight restoration. A multidisciplinary team was vital to ensure this patient's adherence to treatment. With this case, we hope to raise awareness of the deleterious effect on the kidneys from prolonged hypokalemia, the elevated risk of poor renal outcomes in patients with AN-BP, and the danger of easy accessibility to over-the-counter stimulant laxatives.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"16 ","pages":"11795476231169385"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/84/10.1177_11795476231169385.PMC10126689.pdf","citationCount":"0","resultStr":"{\"title\":\"A Multi-Disciplinary Approach to Managing End-Stage Renal Disease in Anorexia Nervosa: A Case Report.\",\"authors\":\"Vishnupriya Khatri, Maryrose Bauschka, Meghan Foley, Cheryl Lundberg, Philip Mehler\",\"doi\":\"10.1177/11795476231169385\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Renal dysfunction and electrolyte abnormalities are common complications of anorexia nervosa (AN), particularly in the binge-eating/purging type (AN-BP). Hypokalemic, or kaliopenic, nephropathy is an established clinical entity and a leading cause of end-stage renal disease (ESRD) in AN. Here, we present a case which demonstrates the difficulties of managing refeeding and nutrition in a psychiatrically and medically complex patient with severe AN-BP and ESRD most likely secondary to hypokalemic nephropathy.</p><p><strong>Case report: </strong>A 54-year-old female with AN-BP that has resulted in chronic hypokalemia, with newly diagnosed ESRD on hemodialysis, presented to an eating disorder medical stabilization unit for weight restoration and treatment of the medical complications associated with her severe malnutrition and ESRD. She was admitted with a body mass index (BMI) of 15 kg/m<sup>2</sup>, serum potassium of 2.8 mmol/L and serum creatinine of 6.91 mg/dL. She had failed to gain weight in the outpatient setting while on hemodialysis. She initially denied having an eating disorder, but ultimately a history of excessive laxative abuse for many years, without primary physician follow up, was revealed. While she did not undergo a renal biopsy to confirm the etiology of her ESRD, given her history of long-standing hypokalemia and lack of other risk factors, her ESRD was presumed to be secondary to hypokalemic nephropathy. She required significant oversight from a multidisciplinary eating disorder treatment team to restore weight while also managing her ESRD.</p><p><strong>Conclusion: </strong>This case report highlights the complexity of managing ESRD in patients with AN who require weight restoration. A multidisciplinary team was vital to ensure this patient's adherence to treatment. With this case, we hope to raise awareness of the deleterious effect on the kidneys from prolonged hypokalemia, the elevated risk of poor renal outcomes in patients with AN-BP, and the danger of easy accessibility to over-the-counter stimulant laxatives.</p>\",\"PeriodicalId\":10357,\"journal\":{\"name\":\"Clinical Medicine Insights. Case Reports\",\"volume\":\"16 \",\"pages\":\"11795476231169385\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/84/10.1177_11795476231169385.PMC10126689.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795476231169385\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476231169385","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
A Multi-Disciplinary Approach to Managing End-Stage Renal Disease in Anorexia Nervosa: A Case Report.
Background: Renal dysfunction and electrolyte abnormalities are common complications of anorexia nervosa (AN), particularly in the binge-eating/purging type (AN-BP). Hypokalemic, or kaliopenic, nephropathy is an established clinical entity and a leading cause of end-stage renal disease (ESRD) in AN. Here, we present a case which demonstrates the difficulties of managing refeeding and nutrition in a psychiatrically and medically complex patient with severe AN-BP and ESRD most likely secondary to hypokalemic nephropathy.
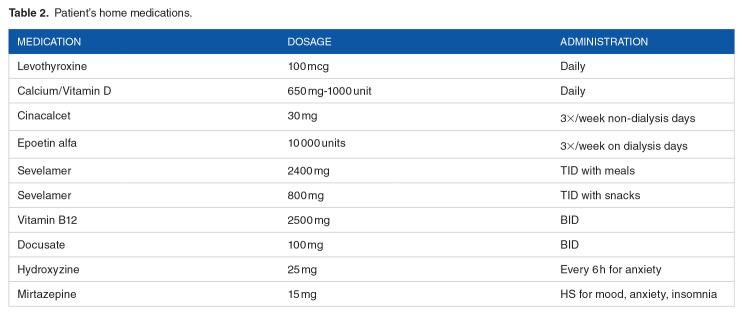
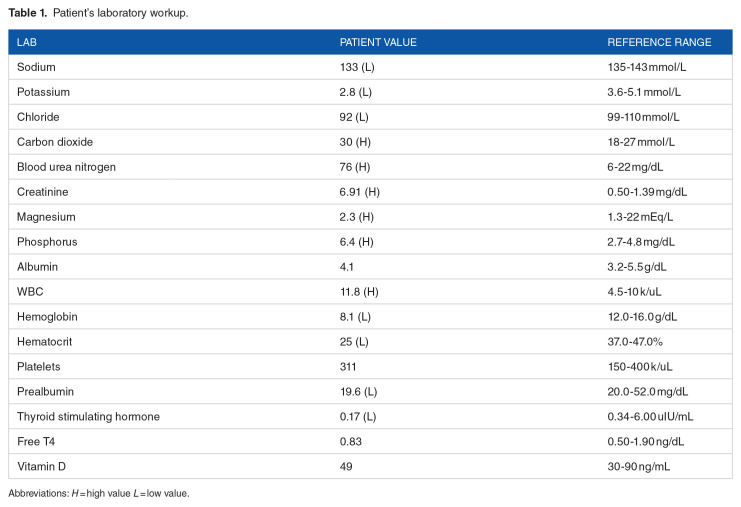
Case report: A 54-year-old female with AN-BP that has resulted in chronic hypokalemia, with newly diagnosed ESRD on hemodialysis, presented to an eating disorder medical stabilization unit for weight restoration and treatment of the medical complications associated with her severe malnutrition and ESRD. She was admitted with a body mass index (BMI) of 15 kg/m2, serum potassium of 2.8 mmol/L and serum creatinine of 6.91 mg/dL. She had failed to gain weight in the outpatient setting while on hemodialysis. She initially denied having an eating disorder, but ultimately a history of excessive laxative abuse for many years, without primary physician follow up, was revealed. While she did not undergo a renal biopsy to confirm the etiology of her ESRD, given her history of long-standing hypokalemia and lack of other risk factors, her ESRD was presumed to be secondary to hypokalemic nephropathy. She required significant oversight from a multidisciplinary eating disorder treatment team to restore weight while also managing her ESRD.
Conclusion: This case report highlights the complexity of managing ESRD in patients with AN who require weight restoration. A multidisciplinary team was vital to ensure this patient's adherence to treatment. With this case, we hope to raise awareness of the deleterious effect on the kidneys from prolonged hypokalemia, the elevated risk of poor renal outcomes in patients with AN-BP, and the danger of easy accessibility to over-the-counter stimulant laxatives.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


