Wonjin Jang, Suejung Jo, Jae Won Yoo, Seongkoo Kim, Jae Wook Lee, Pil-Sang Jang, Nack-Gyun Chung, Bin Cho
{"title":"全身照射剂量对小儿急性淋巴细胞白血病异基因造血干细胞移植第二次完全缓解患者预后的影响。","authors":"Wonjin Jang, Suejung Jo, Jae Won Yoo, Seongkoo Kim, Jae Wook Lee, Pil-Sang Jang, Nack-Gyun Chung, Bin Cho","doi":"10.5045/br.2022.2022174","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Allogeneic HSCT may improve survival in pediatric ALL patients who relapse. In this study, we analyzed the outcome and prognostic factors of 62 ALL patients (35 male, 56.5%) who received allogeneic HSCT in second complete remission (CR) at our institution between April 1st 2009 and December 31st 2019.</p><p><strong>Methods: </strong>The median time from diagnosis to relapse was 35.1 months (range, 6.0‒113.6 mo). Fifty-three patients (85.5%) experienced bone marrow relapse only. The number of patients who received transplant according to each donor type was as follows: HLA matched family donor 17 (27.4%), matched unrelated donor (UD) 22 (35.5%), mismatched donor 23 (37.1%). All patients received HSCT with a myeloablative conditioning, 58 patients (93.5%) with the incorporation of TBI [31 patients 12 Gray (Gy), 24 patients 13.2 Gy, 3 patients 8 Gy].</p><p><strong>Results: </strong>The 5-year event-free survival (EFS), and overall survival of the study group was 41.3±6.3% (26/62), and 42.3±6.6% (27/62), respectively. The cumulative incidence of relapse and transplant-related mortality was 57.1±6.4% and 1.6±1.6%, respectively. Infant ALL, shorter time from diagnosis to relapse, and TBI dose of 12 Gy, rather than 13.2 Gy, resulted in significantly worse EFS. In multivariate analysis, infant ALL and TBI dose of 12 Gy during conditioning predicted significantly lower EFS.</p><p><strong>Conclusion: </strong>In our study group, treatment with a higher dose of TBI during conditioning resulted in better EFS for ALL patients who underwent HSCT in second CR. Further study is needed to determine potential long-term complications associated with a higher TBI dose.</p>","PeriodicalId":46224,"journal":{"name":"Blood Research","volume":"57 4","pages":"256-263"},"PeriodicalIF":2.3000,"publicationDate":"2022-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/06/br-57-4-256.PMC9812732.pdf","citationCount":"0","resultStr":"{\"title\":\"Prognostic impact of total body irradiation dose in pediatric acute lymphoblastic leukemia patients treated with allogeneic hematopoietic stem cell transplantation in second complete remission.\",\"authors\":\"Wonjin Jang, Suejung Jo, Jae Won Yoo, Seongkoo Kim, Jae Wook Lee, Pil-Sang Jang, Nack-Gyun Chung, Bin Cho\",\"doi\":\"10.5045/br.2022.2022174\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Allogeneic HSCT may improve survival in pediatric ALL patients who relapse. In this study, we analyzed the outcome and prognostic factors of 62 ALL patients (35 male, 56.5%) who received allogeneic HSCT in second complete remission (CR) at our institution between April 1st 2009 and December 31st 2019.</p><p><strong>Methods: </strong>The median time from diagnosis to relapse was 35.1 months (range, 6.0‒113.6 mo). Fifty-three patients (85.5%) experienced bone marrow relapse only. The number of patients who received transplant according to each donor type was as follows: HLA matched family donor 17 (27.4%), matched unrelated donor (UD) 22 (35.5%), mismatched donor 23 (37.1%). All patients received HSCT with a myeloablative conditioning, 58 patients (93.5%) with the incorporation of TBI [31 patients 12 Gray (Gy), 24 patients 13.2 Gy, 3 patients 8 Gy].</p><p><strong>Results: </strong>The 5-year event-free survival (EFS), and overall survival of the study group was 41.3±6.3% (26/62), and 42.3±6.6% (27/62), respectively. The cumulative incidence of relapse and transplant-related mortality was 57.1±6.4% and 1.6±1.6%, respectively. Infant ALL, shorter time from diagnosis to relapse, and TBI dose of 12 Gy, rather than 13.2 Gy, resulted in significantly worse EFS. In multivariate analysis, infant ALL and TBI dose of 12 Gy during conditioning predicted significantly lower EFS.</p><p><strong>Conclusion: </strong>In our study group, treatment with a higher dose of TBI during conditioning resulted in better EFS for ALL patients who underwent HSCT in second CR. Further study is needed to determine potential long-term complications associated with a higher TBI dose.</p>\",\"PeriodicalId\":46224,\"journal\":{\"name\":\"Blood Research\",\"volume\":\"57 4\",\"pages\":\"256-263\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-12-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/06/br-57-4-256.PMC9812732.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/br.2022.2022174\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/br.2022.2022174","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Prognostic impact of total body irradiation dose in pediatric acute lymphoblastic leukemia patients treated with allogeneic hematopoietic stem cell transplantation in second complete remission.
Background: Allogeneic HSCT may improve survival in pediatric ALL patients who relapse. In this study, we analyzed the outcome and prognostic factors of 62 ALL patients (35 male, 56.5%) who received allogeneic HSCT in second complete remission (CR) at our institution between April 1st 2009 and December 31st 2019.
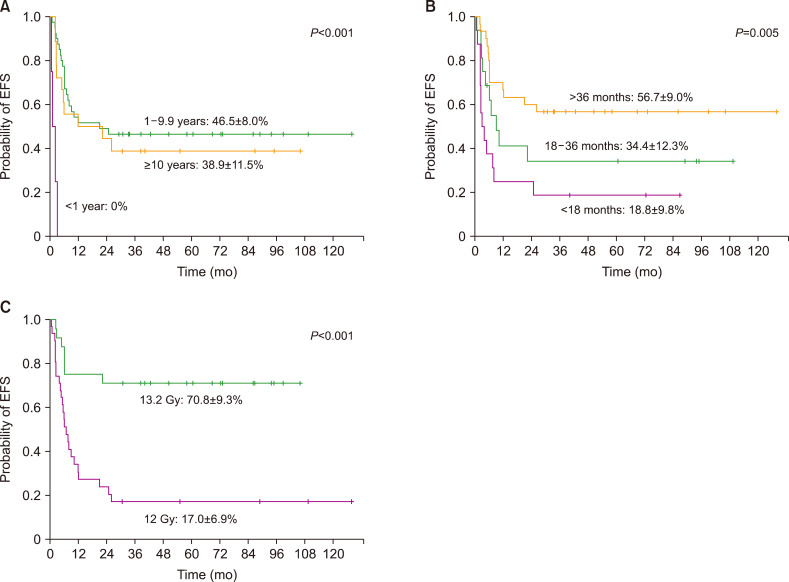
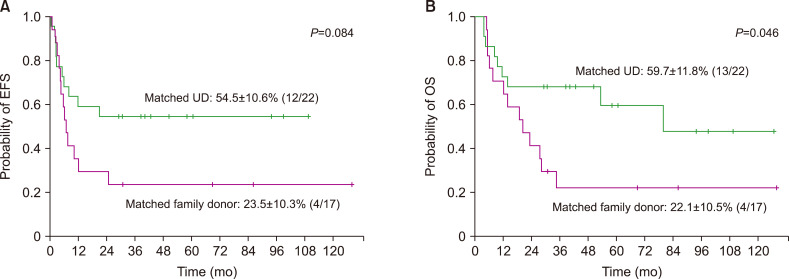
Methods: The median time from diagnosis to relapse was 35.1 months (range, 6.0‒113.6 mo). Fifty-three patients (85.5%) experienced bone marrow relapse only. The number of patients who received transplant according to each donor type was as follows: HLA matched family donor 17 (27.4%), matched unrelated donor (UD) 22 (35.5%), mismatched donor 23 (37.1%). All patients received HSCT with a myeloablative conditioning, 58 patients (93.5%) with the incorporation of TBI [31 patients 12 Gray (Gy), 24 patients 13.2 Gy, 3 patients 8 Gy].
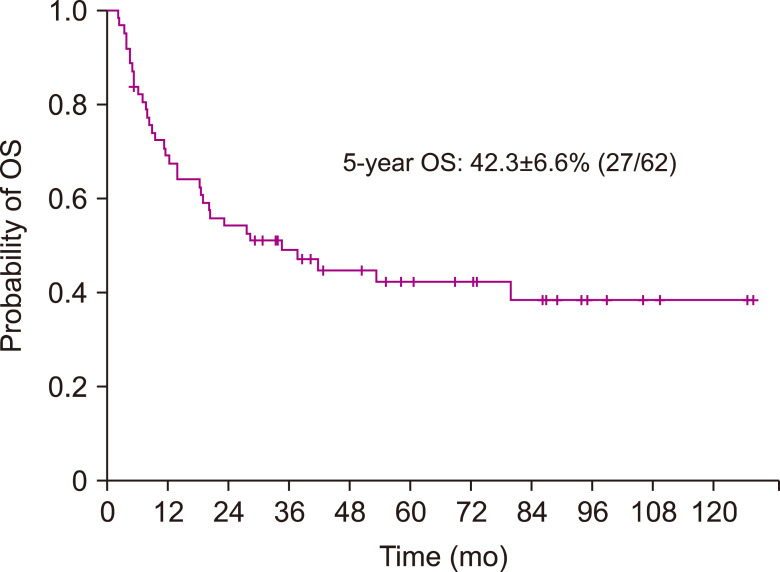
Results: The 5-year event-free survival (EFS), and overall survival of the study group was 41.3±6.3% (26/62), and 42.3±6.6% (27/62), respectively. The cumulative incidence of relapse and transplant-related mortality was 57.1±6.4% and 1.6±1.6%, respectively. Infant ALL, shorter time from diagnosis to relapse, and TBI dose of 12 Gy, rather than 13.2 Gy, resulted in significantly worse EFS. In multivariate analysis, infant ALL and TBI dose of 12 Gy during conditioning predicted significantly lower EFS.
Conclusion: In our study group, treatment with a higher dose of TBI during conditioning resulted in better EFS for ALL patients who underwent HSCT in second CR. Further study is needed to determine potential long-term complications associated with a higher TBI dose.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


