Assen Mladenov, Katharina Diehl, Oliver Müller, Christian von Heymann, Susanne Kopp, Wiebke K Peitsch
{"title":"高压氧治疗和不高压氧治疗坏死性筋膜炎和富尼耶坏疽的预后:10年的回顾性分析。","authors":"Assen Mladenov, Katharina Diehl, Oliver Müller, Christian von Heymann, Susanne Kopp, Wiebke K Peitsch","doi":"10.1186/s13017-022-00448-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Necrotizing soft tissue infections (NSTI) require immediate radical debridement, broad-spectrum antibiotics and intensive care. Hyperbaric oxygen therapy (HBOT) may be performed adjunctively, but unequivocal evidence for its benefits is still lacking.</p><p><strong>Methods: </strong>We performed a retrospective single-center study including 192 patients with necrotizing fasciitis or Fournier's gangrene to assess in-hospital mortality and outcome dependent on patient, disease and treatment characteristics with or without HBOT.</p><p><strong>Results: </strong>The in-hospital mortality rate was 27.6%. Factors associated with increased mortality according to multivariate analysis were higher age, affection of multiple or problem localizations (odds ratio (OR) = 2.88, P = 0.003), ineligibility for HBOT despite clinical indication (OR = 8.59, P = 0.005), pathogens in blood cultures (OR = 3.36, P = 0.002), complications (OR = 10.35, P < 0.001) and sepsis/organ dysfunction (OR = 19.58, P < 0.001). Factors associated with better survival included vacuum-assisted wound closure (OR = 0.17, P < 0.001), larger number of debridements (OR = 0.83, P < 0.001) and defect closure with mesh graft (OR = 0.06, P < 0.001) or flap (OR = 0.09, P = 0.024). When participants were stratified into subgroups without requirement of HBOT (n = 98), treated with HBOT (n = 83) and ineligible for HBOT due to contraindications (n = 11), the first two groups had similar survival rates (75.5% vs. 73.5%) and comparable outcome, although patients with HBOT suffered from more severe NSTI, reflected by more frequent affection of multiple localizations (P < 0.001), sepsis at admission (P < 0.001) and intensive care treatment (P < 0.001), more debridements (P < 0.001) and a larger number of antibiotics (P = 0.001). In the subgroup ineligible for HBOT, survival was significantly worse (36.4%, P = 0.022).</p><p><strong>Conclusion: </strong>These results point to a benefit from HBOT for treatment of NSTI in critically ill patients.</p>","PeriodicalId":290899,"journal":{"name":"World Journal of Emergency Surgery : WJES","volume":" ","pages":"43"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9356491/pdf/","citationCount":"5","resultStr":"{\"title\":\"Outcome of necrotizing fasciitis and Fournier's gangrene with and without hyperbaric oxygen therapy: a retrospective analysis over 10 years.\",\"authors\":\"Assen Mladenov, Katharina Diehl, Oliver Müller, Christian von Heymann, Susanne Kopp, Wiebke K Peitsch\",\"doi\":\"10.1186/s13017-022-00448-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Necrotizing soft tissue infections (NSTI) require immediate radical debridement, broad-spectrum antibiotics and intensive care. Hyperbaric oxygen therapy (HBOT) may be performed adjunctively, but unequivocal evidence for its benefits is still lacking.</p><p><strong>Methods: </strong>We performed a retrospective single-center study including 192 patients with necrotizing fasciitis or Fournier's gangrene to assess in-hospital mortality and outcome dependent on patient, disease and treatment characteristics with or without HBOT.</p><p><strong>Results: </strong>The in-hospital mortality rate was 27.6%. Factors associated with increased mortality according to multivariate analysis were higher age, affection of multiple or problem localizations (odds ratio (OR) = 2.88, P = 0.003), ineligibility for HBOT despite clinical indication (OR = 8.59, P = 0.005), pathogens in blood cultures (OR = 3.36, P = 0.002), complications (OR = 10.35, P < 0.001) and sepsis/organ dysfunction (OR = 19.58, P < 0.001). Factors associated with better survival included vacuum-assisted wound closure (OR = 0.17, P < 0.001), larger number of debridements (OR = 0.83, P < 0.001) and defect closure with mesh graft (OR = 0.06, P < 0.001) or flap (OR = 0.09, P = 0.024). When participants were stratified into subgroups without requirement of HBOT (n = 98), treated with HBOT (n = 83) and ineligible for HBOT due to contraindications (n = 11), the first two groups had similar survival rates (75.5% vs. 73.5%) and comparable outcome, although patients with HBOT suffered from more severe NSTI, reflected by more frequent affection of multiple localizations (P < 0.001), sepsis at admission (P < 0.001) and intensive care treatment (P < 0.001), more debridements (P < 0.001) and a larger number of antibiotics (P = 0.001). In the subgroup ineligible for HBOT, survival was significantly worse (36.4%, P = 0.022).</p><p><strong>Conclusion: </strong>These results point to a benefit from HBOT for treatment of NSTI in critically ill patients.</p>\",\"PeriodicalId\":290899,\"journal\":{\"name\":\"World Journal of Emergency Surgery : WJES\",\"volume\":\" \",\"pages\":\"43\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9356491/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Emergency Surgery : WJES\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13017-022-00448-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery : WJES","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-022-00448-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
摘要
背景:坏死性软组织感染(NSTI)需要立即彻底清创,广谱抗生素和重症监护。高压氧治疗(HBOT)可作为辅助治疗,但其益处仍缺乏明确的证据。方法:我们进行了一项回顾性单中心研究,包括192例坏死性筋膜炎或富尼耶坏疽患者,以评估住院死亡率和结果取决于患者、疾病和治疗特征,有无HBOT。结果:住院死亡率为27.6%。多因素分析显示,与死亡率增加相关的因素有年龄较大、多部位或问题定位的影响(比值比(or) = 2.88, P = 0.003)、尽管有临床指征但不适合使用HBOT (or = 8.59, P = 0.005)、血培养病原体(or = 3.36, P = 0.002)、并发症(or = 10.35, P)。结论:这些结果表明HBOT治疗危重患者NSTI有益处。
Outcome of necrotizing fasciitis and Fournier's gangrene with and without hyperbaric oxygen therapy: a retrospective analysis over 10 years.
Background: Necrotizing soft tissue infections (NSTI) require immediate radical debridement, broad-spectrum antibiotics and intensive care. Hyperbaric oxygen therapy (HBOT) may be performed adjunctively, but unequivocal evidence for its benefits is still lacking.
Methods: We performed a retrospective single-center study including 192 patients with necrotizing fasciitis or Fournier's gangrene to assess in-hospital mortality and outcome dependent on patient, disease and treatment characteristics with or without HBOT.
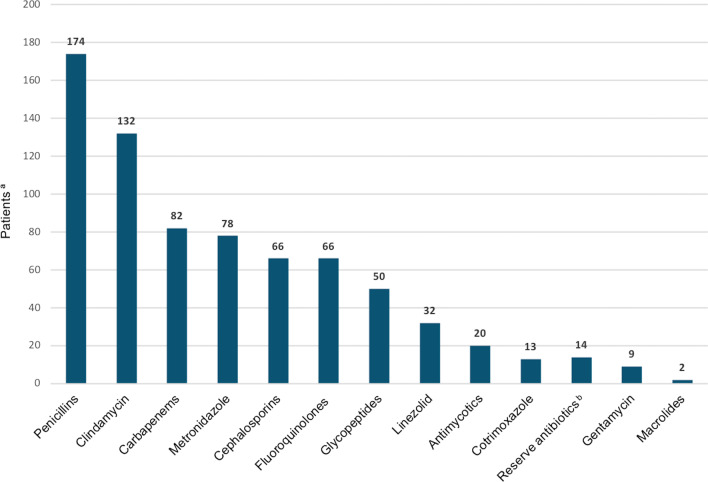
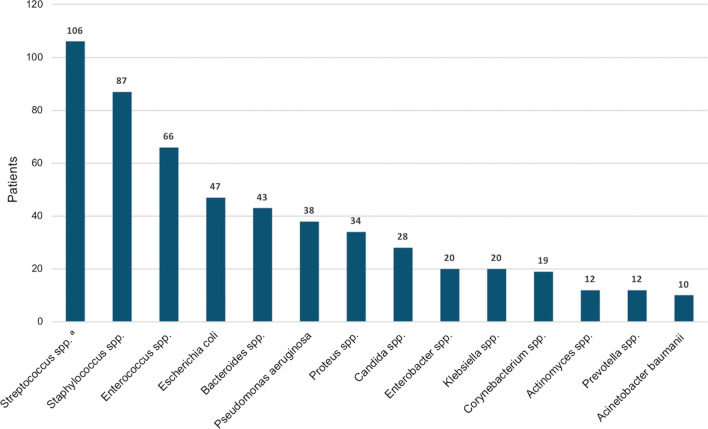
Results: The in-hospital mortality rate was 27.6%. Factors associated with increased mortality according to multivariate analysis were higher age, affection of multiple or problem localizations (odds ratio (OR) = 2.88, P = 0.003), ineligibility for HBOT despite clinical indication (OR = 8.59, P = 0.005), pathogens in blood cultures (OR = 3.36, P = 0.002), complications (OR = 10.35, P < 0.001) and sepsis/organ dysfunction (OR = 19.58, P < 0.001). Factors associated with better survival included vacuum-assisted wound closure (OR = 0.17, P < 0.001), larger number of debridements (OR = 0.83, P < 0.001) and defect closure with mesh graft (OR = 0.06, P < 0.001) or flap (OR = 0.09, P = 0.024). When participants were stratified into subgroups without requirement of HBOT (n = 98), treated with HBOT (n = 83) and ineligible for HBOT due to contraindications (n = 11), the first two groups had similar survival rates (75.5% vs. 73.5%) and comparable outcome, although patients with HBOT suffered from more severe NSTI, reflected by more frequent affection of multiple localizations (P < 0.001), sepsis at admission (P < 0.001) and intensive care treatment (P < 0.001), more debridements (P < 0.001) and a larger number of antibiotics (P = 0.001). In the subgroup ineligible for HBOT, survival was significantly worse (36.4%, P = 0.022).
Conclusion: These results point to a benefit from HBOT for treatment of NSTI in critically ill patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


