Jatinder Singh Sidhu, Geir Salte, Ida Skovgaard Christiansen, Therese Marie Henriette Naur, Asbjørn Høegholm, Paul Frost Clementsen, Uffe Bodtger
{"title":"透视引导下经皮穿刺活检联合支气管镜及支气管内超声诊断可疑肺病变-三合一入路。","authors":"Jatinder Singh Sidhu, Geir Salte, Ida Skovgaard Christiansen, Therese Marie Henriette Naur, Asbjørn Høegholm, Paul Frost Clementsen, Uffe Bodtger","doi":"10.1080/20018525.2020.1723303","DOIUrl":null,"url":null,"abstract":"<p><p>Flexible bronchoscopy and endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TBNA) are the pulmonologists´ basic procedures for the biopsy of suspicious lung lesions. If inconclusive, other guiding-modalities for tissue sampling are needed, computed tomography performed by a radiologist, or - if available - radial EBUS or electromagnetic navigation biopsy. We wanted to investigate if same-day X-ray fluoroscopy-guided transthoracic fine-needle aspiration biopsy (F-TTNAB) performed by the pulmonologist immediately after bronchoscopy and EBUS is a feasible alternative. We retrospectively identified consecutive patients in whom F-TTNAB followed a bronchoscopy and EBUS in the same séance. Patients in whom the suspicion of malignancy was invalidated after complete work up were followed for six months to identify false-negative cases. In total 125 patients underwent triple approach (bronchoscopy, EBUS and F-TTNAB) during the same séance. Malignancy was diagnosed in 86 (69%), and 77 of these (90%) were primary lung cancers. The diagnostic yield of F-TTNAB for malignancy was 77%, and sensitivity was 90%. Pneumothorax occurred in 35 (28%) patients, and was administered with pleural drainage in 22 (18% of all patients). No cases of prolonged haemoptysis were observed. The risk of pneumothorax differed insignificantly with lesion size ≤2.0 cm (27%) <i>versus</i> >2.0 cm (29%). We conclude that it is feasible for pulmonologist to perform F-TTNAB immediately after endoscopy as a combined triple approach in a fast-track workup of suspected lung cancer.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"7 1","pages":"1723303"},"PeriodicalIF":1.8000,"publicationDate":"2020-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/20018525.2020.1723303","citationCount":"6","resultStr":"{\"title\":\"Fluoroscopy guided percutaneous biopsy in combination with bronchoscopy and endobronchial ultrasound in the diagnosis of suspicious lung lesions - the triple approach.\",\"authors\":\"Jatinder Singh Sidhu, Geir Salte, Ida Skovgaard Christiansen, Therese Marie Henriette Naur, Asbjørn Høegholm, Paul Frost Clementsen, Uffe Bodtger\",\"doi\":\"10.1080/20018525.2020.1723303\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Flexible bronchoscopy and endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TBNA) are the pulmonologists´ basic procedures for the biopsy of suspicious lung lesions. If inconclusive, other guiding-modalities for tissue sampling are needed, computed tomography performed by a radiologist, or - if available - radial EBUS or electromagnetic navigation biopsy. We wanted to investigate if same-day X-ray fluoroscopy-guided transthoracic fine-needle aspiration biopsy (F-TTNAB) performed by the pulmonologist immediately after bronchoscopy and EBUS is a feasible alternative. We retrospectively identified consecutive patients in whom F-TTNAB followed a bronchoscopy and EBUS in the same séance. Patients in whom the suspicion of malignancy was invalidated after complete work up were followed for six months to identify false-negative cases. In total 125 patients underwent triple approach (bronchoscopy, EBUS and F-TTNAB) during the same séance. Malignancy was diagnosed in 86 (69%), and 77 of these (90%) were primary lung cancers. The diagnostic yield of F-TTNAB for malignancy was 77%, and sensitivity was 90%. Pneumothorax occurred in 35 (28%) patients, and was administered with pleural drainage in 22 (18% of all patients). No cases of prolonged haemoptysis were observed. The risk of pneumothorax differed insignificantly with lesion size ≤2.0 cm (27%) <i>versus</i> >2.0 cm (29%). We conclude that it is feasible for pulmonologist to perform F-TTNAB immediately after endoscopy as a combined triple approach in a fast-track workup of suspected lung cancer.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"7 1\",\"pages\":\"1723303\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-02-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1080/20018525.2020.1723303\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2020.1723303\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2020.1723303","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Fluoroscopy guided percutaneous biopsy in combination with bronchoscopy and endobronchial ultrasound in the diagnosis of suspicious lung lesions - the triple approach.
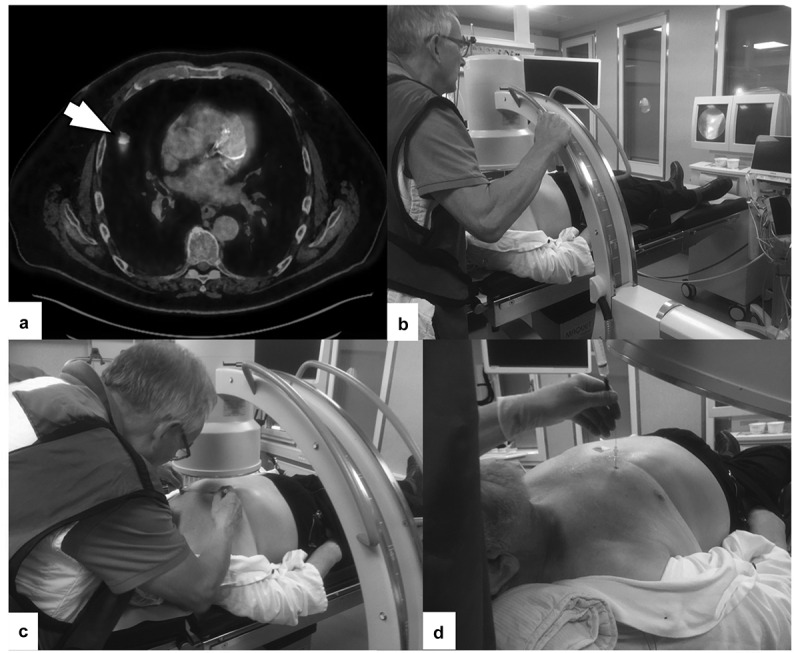
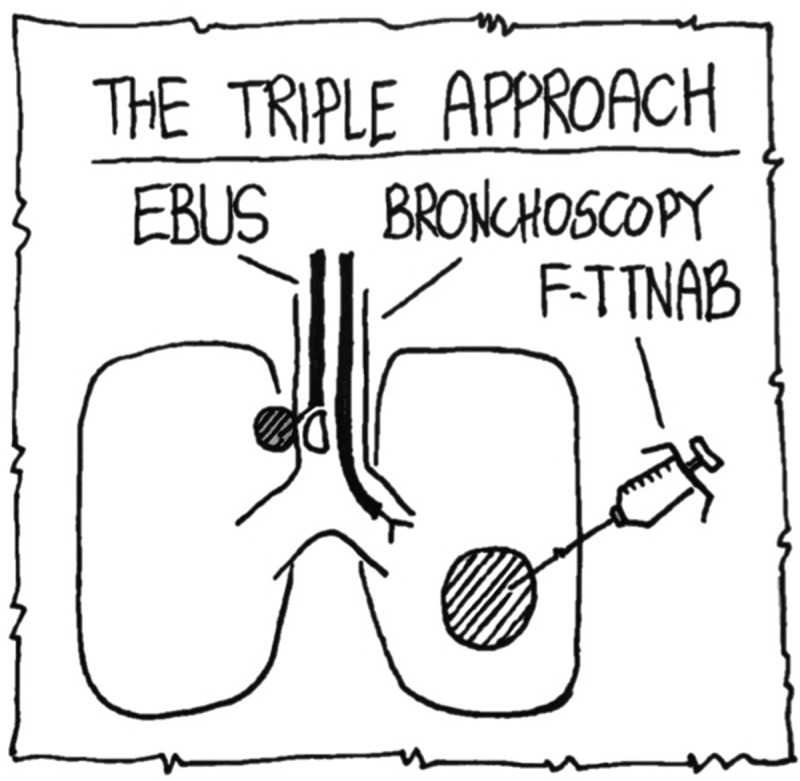
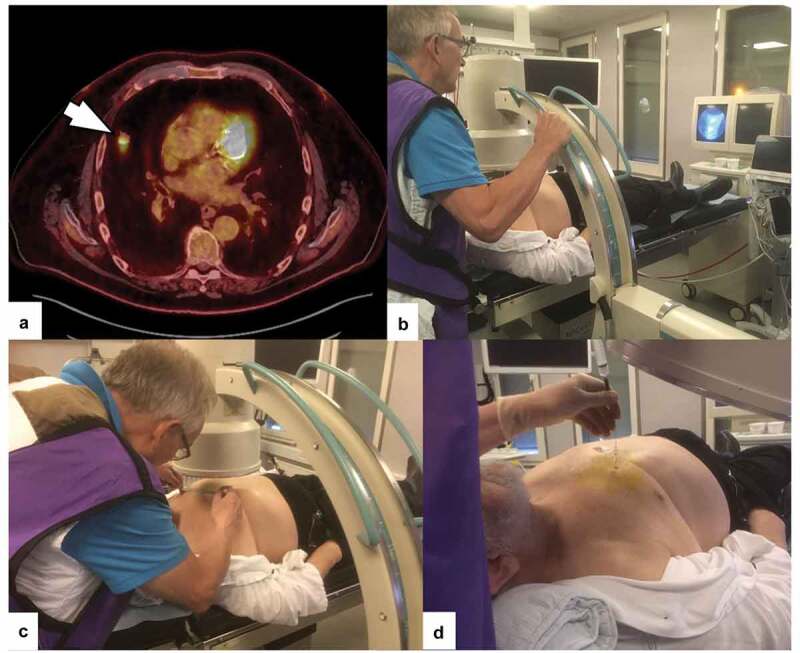
Flexible bronchoscopy and endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TBNA) are the pulmonologists´ basic procedures for the biopsy of suspicious lung lesions. If inconclusive, other guiding-modalities for tissue sampling are needed, computed tomography performed by a radiologist, or - if available - radial EBUS or electromagnetic navigation biopsy. We wanted to investigate if same-day X-ray fluoroscopy-guided transthoracic fine-needle aspiration biopsy (F-TTNAB) performed by the pulmonologist immediately after bronchoscopy and EBUS is a feasible alternative. We retrospectively identified consecutive patients in whom F-TTNAB followed a bronchoscopy and EBUS in the same séance. Patients in whom the suspicion of malignancy was invalidated after complete work up were followed for six months to identify false-negative cases. In total 125 patients underwent triple approach (bronchoscopy, EBUS and F-TTNAB) during the same séance. Malignancy was diagnosed in 86 (69%), and 77 of these (90%) were primary lung cancers. The diagnostic yield of F-TTNAB for malignancy was 77%, and sensitivity was 90%. Pneumothorax occurred in 35 (28%) patients, and was administered with pleural drainage in 22 (18% of all patients). No cases of prolonged haemoptysis were observed. The risk of pneumothorax differed insignificantly with lesion size ≤2.0 cm (27%) versus >2.0 cm (29%). We conclude that it is feasible for pulmonologist to perform F-TTNAB immediately after endoscopy as a combined triple approach in a fast-track workup of suspected lung cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


