{"title":"2型和3型胃神经内分泌肿瘤淋巴结转移风险高:系统回顾和荟萃分析","authors":"Yohei Ogata, Waku Hatta, Takeshi Kanno, Masahiro Saito, Xiaoyi Jin, Naoki Asano, Tomoyuki Koike, Akira Imatani, Yuhong Yuan, Atsushi Masamune","doi":"10.1111/den.15026","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Lymph node metastasis (LNM) is crucial in determining treatment strategies for gastric neuroendocrine tumors (gNETs). While type 3 is considered more aggressive than types 1 and 2 within the clinical subtype of gNETs, the supporting data were insufficient, due to their rarity. We aimed to study the prevalence and risk factors associated with LNM in gNETs.</p><p><strong>Methods: </strong>We searched electronic databases from 1990 to 2023 to identify case-control and cohort studies regarding gNETs resected either endoscopically or surgically. The primary outcome measured was the pooled prevalence of LNM in gNETs. Secondary outcomes included categorizing the prevalence of LNM by clinical subtypes and identifying pathological risk factors associated with LNM in gNETs.</p><p><strong>Results: </strong>We included 28 studies, involving 1742 patients, among whom 240 had LNM (pooled prevalence rate, 11.8%; 95% confidence interval 7.6-17.9%). The pooled prevalence rates of LNM for type 1, type 2, and type 3 gNETs were 6.0%, 38.5%, and 23.2%, respectively. Type 2 (odds ratio [95% confidence interval] 11.53 [3.46-38.49]) and type 3 (6.88 [3.79-12.49]) gNETs exhibited a higher risk for LNM compared to type 1. Pathological risk factors for LNM included tumor size >10 mm (4.18 [1.91-9.17]), tumor invasion into the muscularis propria or deeper (11.21 [3.50-35.92]), grade 2/grade 3 (5.96 [2.65-13.40]), and lymphovascular invasion (34.50 [6.70-177.51]).</p><p><strong>Conclusion: </strong>We demonstrated that type 2 gNETs, as well as type 3, had a high risk of LNM. Additionally, four pathological risk factors associated with LNM were identified.</p>","PeriodicalId":72813,"journal":{"name":"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society","volume":" ","pages":"834-843"},"PeriodicalIF":4.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333324/pdf/","citationCount":"0","resultStr":"{\"title\":\"Type 2 and type 3 gastric neuroendocrine tumors have high risk of lymph node metastasis: Systematic review and meta-analysis.\",\"authors\":\"Yohei Ogata, Waku Hatta, Takeshi Kanno, Masahiro Saito, Xiaoyi Jin, Naoki Asano, Tomoyuki Koike, Akira Imatani, Yuhong Yuan, Atsushi Masamune\",\"doi\":\"10.1111/den.15026\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Lymph node metastasis (LNM) is crucial in determining treatment strategies for gastric neuroendocrine tumors (gNETs). While type 3 is considered more aggressive than types 1 and 2 within the clinical subtype of gNETs, the supporting data were insufficient, due to their rarity. We aimed to study the prevalence and risk factors associated with LNM in gNETs.</p><p><strong>Methods: </strong>We searched electronic databases from 1990 to 2023 to identify case-control and cohort studies regarding gNETs resected either endoscopically or surgically. The primary outcome measured was the pooled prevalence of LNM in gNETs. Secondary outcomes included categorizing the prevalence of LNM by clinical subtypes and identifying pathological risk factors associated with LNM in gNETs.</p><p><strong>Results: </strong>We included 28 studies, involving 1742 patients, among whom 240 had LNM (pooled prevalence rate, 11.8%; 95% confidence interval 7.6-17.9%). The pooled prevalence rates of LNM for type 1, type 2, and type 3 gNETs were 6.0%, 38.5%, and 23.2%, respectively. Type 2 (odds ratio [95% confidence interval] 11.53 [3.46-38.49]) and type 3 (6.88 [3.79-12.49]) gNETs exhibited a higher risk for LNM compared to type 1. Pathological risk factors for LNM included tumor size >10 mm (4.18 [1.91-9.17]), tumor invasion into the muscularis propria or deeper (11.21 [3.50-35.92]), grade 2/grade 3 (5.96 [2.65-13.40]), and lymphovascular invasion (34.50 [6.70-177.51]).</p><p><strong>Conclusion: </strong>We demonstrated that type 2 gNETs, as well as type 3, had a high risk of LNM. Additionally, four pathological risk factors associated with LNM were identified.</p>\",\"PeriodicalId\":72813,\"journal\":{\"name\":\"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society\",\"volume\":\" \",\"pages\":\"834-843\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333324/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1111/den.15026\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/den.15026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Type 2 and type 3 gastric neuroendocrine tumors have high risk of lymph node metastasis: Systematic review and meta-analysis.
Objectives: Lymph node metastasis (LNM) is crucial in determining treatment strategies for gastric neuroendocrine tumors (gNETs). While type 3 is considered more aggressive than types 1 and 2 within the clinical subtype of gNETs, the supporting data were insufficient, due to their rarity. We aimed to study the prevalence and risk factors associated with LNM in gNETs.
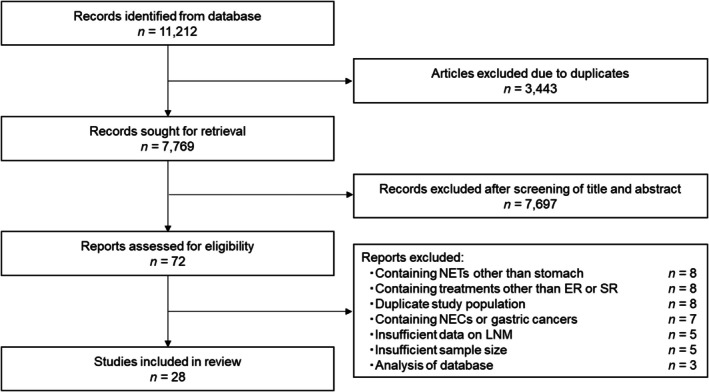
Methods: We searched electronic databases from 1990 to 2023 to identify case-control and cohort studies regarding gNETs resected either endoscopically or surgically. The primary outcome measured was the pooled prevalence of LNM in gNETs. Secondary outcomes included categorizing the prevalence of LNM by clinical subtypes and identifying pathological risk factors associated with LNM in gNETs.
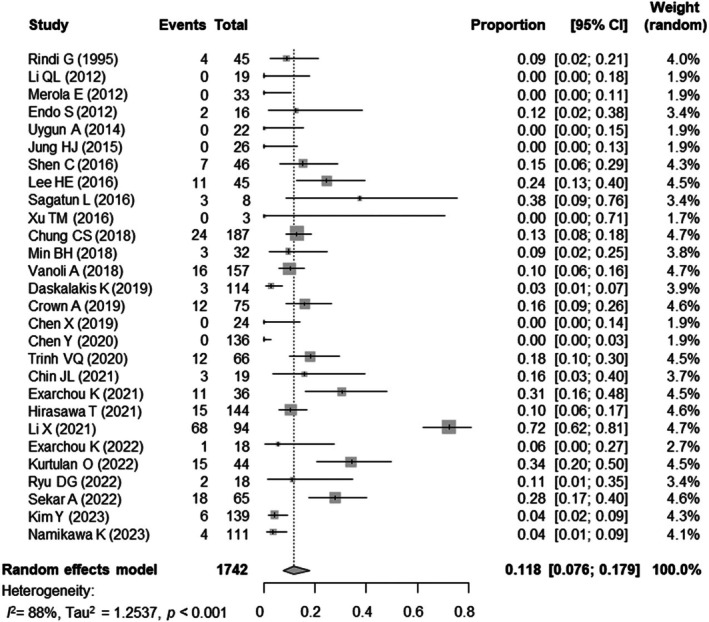
Results: We included 28 studies, involving 1742 patients, among whom 240 had LNM (pooled prevalence rate, 11.8%; 95% confidence interval 7.6-17.9%). The pooled prevalence rates of LNM for type 1, type 2, and type 3 gNETs were 6.0%, 38.5%, and 23.2%, respectively. Type 2 (odds ratio [95% confidence interval] 11.53 [3.46-38.49]) and type 3 (6.88 [3.79-12.49]) gNETs exhibited a higher risk for LNM compared to type 1. Pathological risk factors for LNM included tumor size >10 mm (4.18 [1.91-9.17]), tumor invasion into the muscularis propria or deeper (11.21 [3.50-35.92]), grade 2/grade 3 (5.96 [2.65-13.40]), and lymphovascular invasion (34.50 [6.70-177.51]).
Conclusion: We demonstrated that type 2 gNETs, as well as type 3, had a high risk of LNM. Additionally, four pathological risk factors associated with LNM were identified.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


