Yanik J Bababekov, Anna H Ha, Trevor L Nydam, Carlos Goncalves, Rashikh Choudhury, JoLynn Shinsako, Maria Baimas-George, David M Reynolds, Cassidy Yoshida, Caroline A Racke, Han Grewal, Sophia Pomposelli, Ivan E Rodriguez, Jordan R H Hoffman, Jesse D Schold, Bruce Kaplan, Elizabeth A Pomfret, James J Pomposelli
{"title":"胸腹常温区域灌注:DCD肝移植的现实经验和结果。","authors":"Yanik J Bababekov, Anna H Ha, Trevor L Nydam, Carlos Goncalves, Rashikh Choudhury, JoLynn Shinsako, Maria Baimas-George, David M Reynolds, Cassidy Yoshida, Caroline A Racke, Han Grewal, Sophia Pomposelli, Ivan E Rodriguez, Jordan R H Hoffman, Jesse D Schold, Bruce Kaplan, Elizabeth A Pomfret, James J Pomposelli","doi":"10.1097/TXD.0000000000001767","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Donation after circulatory death liver transplantation (DCD LT) is underused given historical outcomes fraught with ischemic cholangiopathy (IC). We aimed to assess 6-mo IC in LT from DCD via normothermic regional perfusion (NRP) compared with DCD via static cold storage (SCS).</p><p><strong>Methods: </strong>A retrospective review of adult Maastricht-III DCD liver donors and recipients at the University of Colorado Hospital from January 1, 2017, to August 27, 2024, was performed. The 6-mo IC rate was compared between NRP and SCS. Secondary outcomes included biochemical assessments of accepted versus declined NRP liver allografts and allograft and patient survival for NRP and SCS groups.</p><p><strong>Results: </strong>One hundred sixty-two DCD LTs (SCS = 79; NRP = 97) were performed and 150 recipients (SCS = 74; NRP = 86) reached 6-mo follow-up. Six-month IC was lower for NRP compared with SCS (1.2% versus 9.5%, <i>P</i> = 0.03). The Donor Risk Index (2.44 [2.02-2.82] versus 2.17 [1.97-2.30], <i>P</i> = 0.002) and UK DCD Risk Score (4.2 ± 2.9 versus 3.2 ± 2.3, <i>P</i> = 0.008) were higher for NRP versus SCS. The Liver Graft assessment Following Transplantation score was less for NRP compared with SCS (-3.3 versus -3.1, <i>P</i> < 0.05). There were several differences in median biochemical parameters during NRP between accepted and declined livers, including higher terminal biliary bicarbonate (22.7 [20.9-29.1] versus 10.8 [7.6-13.1] mEq/L, <i>P</i> = 0.004). There were no significant differences in 12-mo allograft or patient survival for NRP versus SCS.</p><p><strong>Conclusions: </strong>NRP is a disruptive innovation that improves the utilization of DCD livers. Despite higher-risk donor-recipient pairing for NRP compared with SCS, we demonstrate a decrease in IC for NRP. These data facilitate benchmarking of thoracoabdominal NRP DCD LT and support further protocol development.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 3","pages":"e1767"},"PeriodicalIF":1.9000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11875611/pdf/","citationCount":"0","resultStr":"{\"title\":\"Thoracoabdominal Normothermic Regional Perfusion: Real-world Experience and Outcomes of DCD Liver Transplantation.\",\"authors\":\"Yanik J Bababekov, Anna H Ha, Trevor L Nydam, Carlos Goncalves, Rashikh Choudhury, JoLynn Shinsako, Maria Baimas-George, David M Reynolds, Cassidy Yoshida, Caroline A Racke, Han Grewal, Sophia Pomposelli, Ivan E Rodriguez, Jordan R H Hoffman, Jesse D Schold, Bruce Kaplan, Elizabeth A Pomfret, James J Pomposelli\",\"doi\":\"10.1097/TXD.0000000000001767\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Donation after circulatory death liver transplantation (DCD LT) is underused given historical outcomes fraught with ischemic cholangiopathy (IC). We aimed to assess 6-mo IC in LT from DCD via normothermic regional perfusion (NRP) compared with DCD via static cold storage (SCS).</p><p><strong>Methods: </strong>A retrospective review of adult Maastricht-III DCD liver donors and recipients at the University of Colorado Hospital from January 1, 2017, to August 27, 2024, was performed. The 6-mo IC rate was compared between NRP and SCS. Secondary outcomes included biochemical assessments of accepted versus declined NRP liver allografts and allograft and patient survival for NRP and SCS groups.</p><p><strong>Results: </strong>One hundred sixty-two DCD LTs (SCS = 79; NRP = 97) were performed and 150 recipients (SCS = 74; NRP = 86) reached 6-mo follow-up. Six-month IC was lower for NRP compared with SCS (1.2% versus 9.5%, <i>P</i> = 0.03). The Donor Risk Index (2.44 [2.02-2.82] versus 2.17 [1.97-2.30], <i>P</i> = 0.002) and UK DCD Risk Score (4.2 ± 2.9 versus 3.2 ± 2.3, <i>P</i> = 0.008) were higher for NRP versus SCS. The Liver Graft assessment Following Transplantation score was less for NRP compared with SCS (-3.3 versus -3.1, <i>P</i> < 0.05). There were several differences in median biochemical parameters during NRP between accepted and declined livers, including higher terminal biliary bicarbonate (22.7 [20.9-29.1] versus 10.8 [7.6-13.1] mEq/L, <i>P</i> = 0.004). There were no significant differences in 12-mo allograft or patient survival for NRP versus SCS.</p><p><strong>Conclusions: </strong>NRP is a disruptive innovation that improves the utilization of DCD livers. Despite higher-risk donor-recipient pairing for NRP compared with SCS, we demonstrate a decrease in IC for NRP. These data facilitate benchmarking of thoracoabdominal NRP DCD LT and support further protocol development.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"11 3\",\"pages\":\"e1767\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-02-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11875611/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001767\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001767","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
摘要
背景:鉴于历史结果充满缺血性胆管病(IC),循环死亡肝移植(DCD LT)后的捐赠未得到充分利用。我们的目的是评估通过常温区域灌注(NRP)的DCD与通过静态冷库(SCS)的DCD在LT中的6个月IC。方法:回顾性分析2017年1月1日至2024年8月27日在科罗拉多大学医院进行的成人马斯特里赫特iii型DCD肝脏供体和受体。比较NRP和SCS的6个月IC率。次要结局包括接受与拒绝接受同种异体肝移植的生化评估,以及NRP组和SCS组的患者生存。结果:162例DCD LTs (SCS = 79;NRP = 97), 150例受者(SCS = 74;NRP = 86)随访6个月。与SCS相比,NRP的6个月IC较低(1.2%对9.5%,P = 0.03)。供者风险指数(2.44[2.02-2.82]比2.17 [1.97-2.30],P = 0.002)和UK DCD风险评分(4.2±2.9比3.2±2.3,P = 0.008) NRP高于SCS。与SCS相比,NRP的肝移植后评估评分较低(-3.3 vs -3.1, P P = 0.004)。NRP与SCS在12个月同种异体移植或患者生存方面没有显著差异。结论:NRP是一项颠覆性创新,提高了DCD肝脏的利用率。尽管与SCS相比,NRP的供体-受体配对风险更高,但我们证明了NRP的IC降低。这些数据有助于胸腹NRP DCD LT的基准制定,并支持进一步的方案制定。
Thoracoabdominal Normothermic Regional Perfusion: Real-world Experience and Outcomes of DCD Liver Transplantation.
Background: Donation after circulatory death liver transplantation (DCD LT) is underused given historical outcomes fraught with ischemic cholangiopathy (IC). We aimed to assess 6-mo IC in LT from DCD via normothermic regional perfusion (NRP) compared with DCD via static cold storage (SCS).
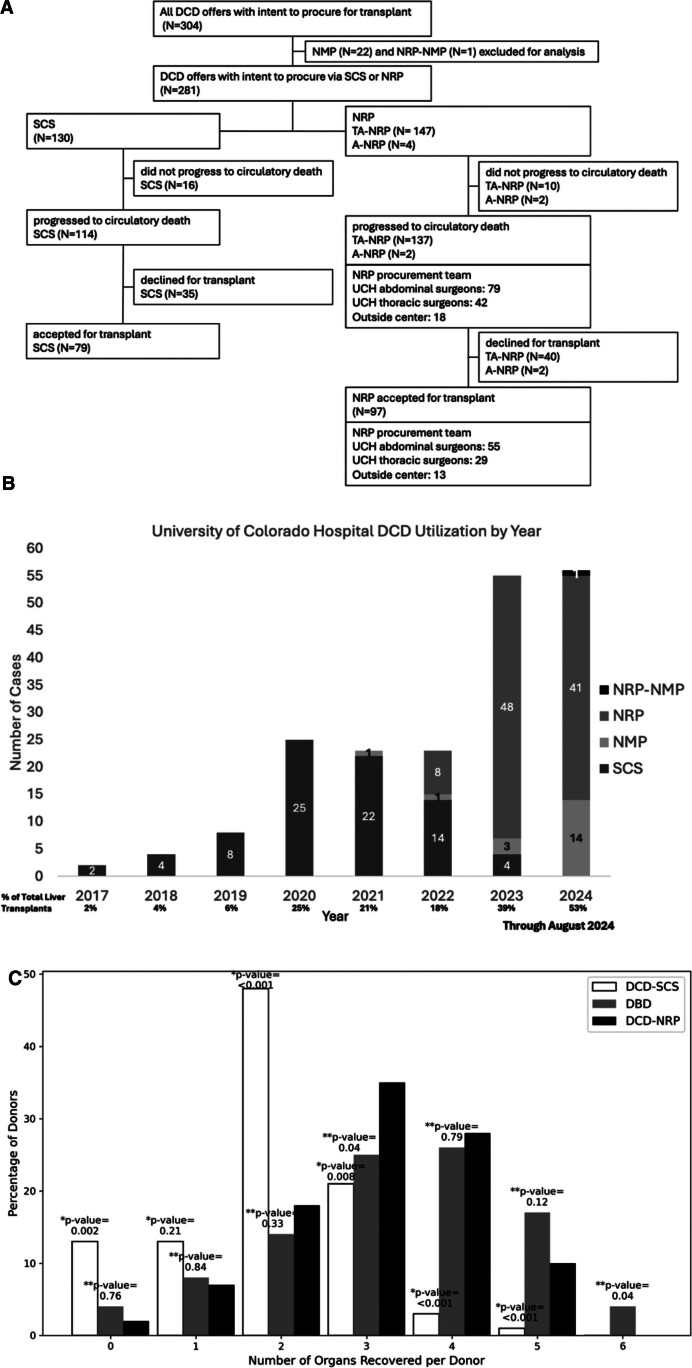
Methods: A retrospective review of adult Maastricht-III DCD liver donors and recipients at the University of Colorado Hospital from January 1, 2017, to August 27, 2024, was performed. The 6-mo IC rate was compared between NRP and SCS. Secondary outcomes included biochemical assessments of accepted versus declined NRP liver allografts and allograft and patient survival for NRP and SCS groups.
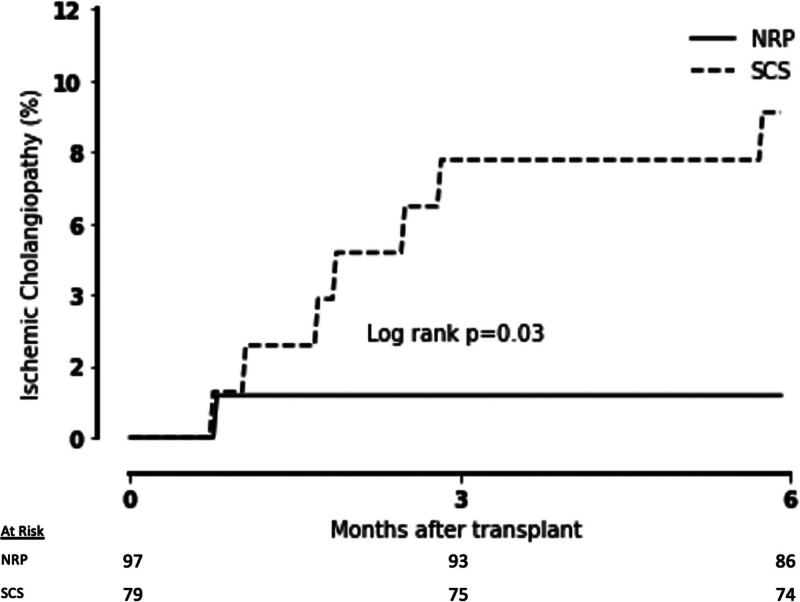
Results: One hundred sixty-two DCD LTs (SCS = 79; NRP = 97) were performed and 150 recipients (SCS = 74; NRP = 86) reached 6-mo follow-up. Six-month IC was lower for NRP compared with SCS (1.2% versus 9.5%, P = 0.03). The Donor Risk Index (2.44 [2.02-2.82] versus 2.17 [1.97-2.30], P = 0.002) and UK DCD Risk Score (4.2 ± 2.9 versus 3.2 ± 2.3, P = 0.008) were higher for NRP versus SCS. The Liver Graft assessment Following Transplantation score was less for NRP compared with SCS (-3.3 versus -3.1, P < 0.05). There were several differences in median biochemical parameters during NRP between accepted and declined livers, including higher terminal biliary bicarbonate (22.7 [20.9-29.1] versus 10.8 [7.6-13.1] mEq/L, P = 0.004). There were no significant differences in 12-mo allograft or patient survival for NRP versus SCS.
Conclusions: NRP is a disruptive innovation that improves the utilization of DCD livers. Despite higher-risk donor-recipient pairing for NRP compared with SCS, we demonstrate a decrease in IC for NRP. These data facilitate benchmarking of thoracoabdominal NRP DCD LT and support further protocol development.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


