Ana Neves, Rita Gouveia, Sérgio Madureira, Catarina Elias, Pedro Ribeirinho-Soares, Marta Soares-Carreira, Joana Pereira, Jorge Almeida, Patrícia Lourenço
{"title":"血小板分布宽度——慢性心力衰竭患者的预后指标。","authors":"Ana Neves, Rita Gouveia, Sérgio Madureira, Catarina Elias, Pedro Ribeirinho-Soares, Marta Soares-Carreira, Joana Pereira, Jorge Almeida, Patrícia Lourenço","doi":"10.1097/j.pbj.0000000000000277","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Increased levels of platelet distribution width (PDW) can predict cardiac death and infarction recurrence in acute myocardial infarction. PDW appears to be a prognosis marker in acute heart failure (HF); however, its impact on chronic HF is still unknown. We investigated the impact of PDW on chronic HF.</p><p><strong>Methods: </strong>We retrospectively analyzed outpatients with chronic HF with left ventricular systolic dysfunction (LVSD) from January 2012 to May 2018. Patients with no data on PDW levels or with preserved or recovered ejection fraction were excluded. The primary end point was all-cause mortality. Multivariable Cox regression analysis was used to evaluate the association between PDW and mortality. A multivariate model was built adjusting for age, sex, comorbidities, brain-type natriuretic peptide, New York Heart Association (NYHA) class, evidence-based therapy, and severity of LVSD.</p><p><strong>Results: </strong>In our cohort of 766 patients, 65.7% were male, the mean age was 70 years, and 35.4% were in NYHA class I; 38.3% had diabetes mellitus, 51.4% had severe LVSD, and 3.9% had an inflammatory or autoimmune disease. The median (interquartile range) PDW was 13.5 (12.1-14.9) fL. During a median follow-up of 49 (30-79) months, 372 patients (48.6%) died. Patients with PDW ≥ 14.3 fL presented a multivariate-adjusted higher risk of all-cause death than those with lower values (hazard ratio: 1.32, 95% confidence interval [CI]: 1.05-1.64, <i>P</i> = .2).</p><p><strong>Conclusions: </strong>Patients with PDW ≥14.3 fL (upper tercile for PDW) presented a multivariate-adjusted 32% (95% CI: 5-64%) higher risk of all-cause death than those with lower values. PDW can help clinicians stratify patients with chronic HF; it is a practical, inexpensive, and widely available parameter.</p>","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"10 1","pages":"277"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11706588/pdf/","citationCount":"0","resultStr":"{\"title\":\"Platelet distribution width-a prognosis marker in patients with chronic heart failure.\",\"authors\":\"Ana Neves, Rita Gouveia, Sérgio Madureira, Catarina Elias, Pedro Ribeirinho-Soares, Marta Soares-Carreira, Joana Pereira, Jorge Almeida, Patrícia Lourenço\",\"doi\":\"10.1097/j.pbj.0000000000000277\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Increased levels of platelet distribution width (PDW) can predict cardiac death and infarction recurrence in acute myocardial infarction. PDW appears to be a prognosis marker in acute heart failure (HF); however, its impact on chronic HF is still unknown. We investigated the impact of PDW on chronic HF.</p><p><strong>Methods: </strong>We retrospectively analyzed outpatients with chronic HF with left ventricular systolic dysfunction (LVSD) from January 2012 to May 2018. Patients with no data on PDW levels or with preserved or recovered ejection fraction were excluded. The primary end point was all-cause mortality. Multivariable Cox regression analysis was used to evaluate the association between PDW and mortality. A multivariate model was built adjusting for age, sex, comorbidities, brain-type natriuretic peptide, New York Heart Association (NYHA) class, evidence-based therapy, and severity of LVSD.</p><p><strong>Results: </strong>In our cohort of 766 patients, 65.7% were male, the mean age was 70 years, and 35.4% were in NYHA class I; 38.3% had diabetes mellitus, 51.4% had severe LVSD, and 3.9% had an inflammatory or autoimmune disease. The median (interquartile range) PDW was 13.5 (12.1-14.9) fL. During a median follow-up of 49 (30-79) months, 372 patients (48.6%) died. Patients with PDW ≥ 14.3 fL presented a multivariate-adjusted higher risk of all-cause death than those with lower values (hazard ratio: 1.32, 95% confidence interval [CI]: 1.05-1.64, <i>P</i> = .2).</p><p><strong>Conclusions: </strong>Patients with PDW ≥14.3 fL (upper tercile for PDW) presented a multivariate-adjusted 32% (95% CI: 5-64%) higher risk of all-cause death than those with lower values. PDW can help clinicians stratify patients with chronic HF; it is a practical, inexpensive, and widely available parameter.</p>\",\"PeriodicalId\":74479,\"journal\":{\"name\":\"Porto biomedical journal\",\"volume\":\"10 1\",\"pages\":\"277\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11706588/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Porto biomedical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/j.pbj.0000000000000277\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000277","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Platelet distribution width-a prognosis marker in patients with chronic heart failure.
Background: Increased levels of platelet distribution width (PDW) can predict cardiac death and infarction recurrence in acute myocardial infarction. PDW appears to be a prognosis marker in acute heart failure (HF); however, its impact on chronic HF is still unknown. We investigated the impact of PDW on chronic HF.
Methods: We retrospectively analyzed outpatients with chronic HF with left ventricular systolic dysfunction (LVSD) from January 2012 to May 2018. Patients with no data on PDW levels or with preserved or recovered ejection fraction were excluded. The primary end point was all-cause mortality. Multivariable Cox regression analysis was used to evaluate the association between PDW and mortality. A multivariate model was built adjusting for age, sex, comorbidities, brain-type natriuretic peptide, New York Heart Association (NYHA) class, evidence-based therapy, and severity of LVSD.
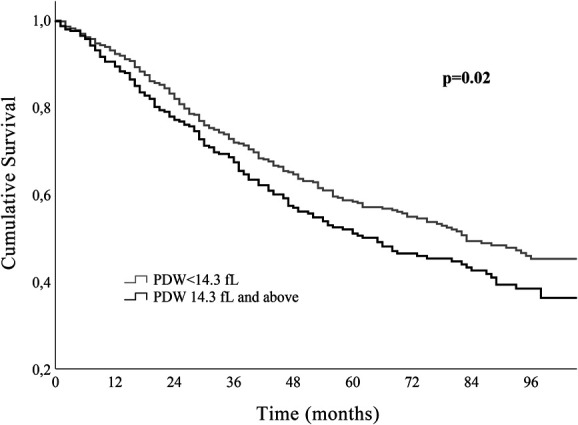
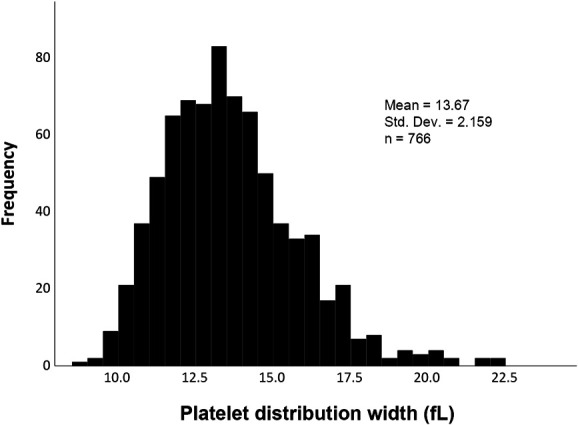
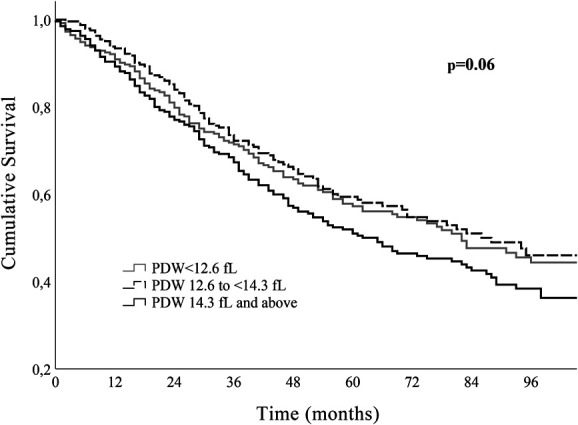
Results: In our cohort of 766 patients, 65.7% were male, the mean age was 70 years, and 35.4% were in NYHA class I; 38.3% had diabetes mellitus, 51.4% had severe LVSD, and 3.9% had an inflammatory or autoimmune disease. The median (interquartile range) PDW was 13.5 (12.1-14.9) fL. During a median follow-up of 49 (30-79) months, 372 patients (48.6%) died. Patients with PDW ≥ 14.3 fL presented a multivariate-adjusted higher risk of all-cause death than those with lower values (hazard ratio: 1.32, 95% confidence interval [CI]: 1.05-1.64, P = .2).
Conclusions: Patients with PDW ≥14.3 fL (upper tercile for PDW) presented a multivariate-adjusted 32% (95% CI: 5-64%) higher risk of all-cause death than those with lower values. PDW can help clinicians stratify patients with chronic HF; it is a practical, inexpensive, and widely available parameter.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


