Fabian Halleck, Georg A. Böhmig, Lionel Couzi, Lionel Rostaing, Gunilla Einecke, Carmen Lefaucheur, Christophe Legendre, Robert Montgomery, Peter Hughes, Anil Chandraker, Kate Wyburn, Phil Halloran, Angela Q. Maldonado, Kristoffer Sjöholm, Anna Runström, Paola Lefèvre, Jan Tollemar, Stanley Jordan
{"title":"比较伊立菲酶和血浆置换术治疗肾移植受者抗体相关排斥反应的随机试验","authors":"Fabian Halleck, Georg A. Böhmig, Lionel Couzi, Lionel Rostaing, Gunilla Einecke, Carmen Lefaucheur, Christophe Legendre, Robert Montgomery, Peter Hughes, Anil Chandraker, Kate Wyburn, Phil Halloran, Angela Q. Maldonado, Kristoffer Sjöholm, Anna Runström, Paola Lefèvre, Jan Tollemar, Stanley Jordan","doi":"10.1111/ctr.15383","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Antibody-mediated rejection (ABMR) poses a barrier to long-term graft survival and is one of the most challenging events after kidney transplantation. Removing donor specific antibodies (DSA) through therapeutic plasma exchange (PLEX) is a cornerstone of antibody depletion but has inconsistent effects. Imlifidase is a treatment currently utilized for desensitization with near-complete inactivation of DSA both in the intra- and extravascular space.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a 6-month, randomized, open-label, multicenter, multinational trial conducted at 14 transplant centers. Thirty patients were randomized to either imlifidase or PLEX treatment. The primary endpoint was reduction in DSA level during the 5 days following the start of treatment.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Despite considerable heterogeneity in the trial population, DSA reduction as defined by the primary endpoint was 97% for imlifidase compared to 42% for PLEX. Additionally, imlifidase reduced DSA to noncomplement fixing levels, whereas PLEX failed to do so. After antibody rebound in the imlifidase arm (circa days 6–12), both arms had similar reductions in DSA. Five allograft losses occurred during the 6 months following the start of ABMR treatment—four within the imlifidase arm (18 patients treated) and one in the PLEX arm (10 patients treated). In terms of clinical efficacy, the Kaplan–Meier estimated graft survival was 78% for imlifidase and 89% for PLEX, with a slightly higher eGFR in the PLEX arm at the end of the trial. The observed adverse events in the trial were as expected, and there were no apparent differences between the arms.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Imlifidase was safe and well-tolerated in the ABMR population. Despite meeting the primary endpoint of maximum DSA reduction compared to PLEX, the trial was unsuccessful in demonstrating a clinical benefit of imlifidase in this heterogenous ABMR population.</p>\n </section>\n \n <section>\n \n <h3> Trial Registration</h3>\n \n <p>EudraCT number: 2018-000022-66, 2020-004777-49; ClinicalTrials.gov identifier: NCT03897205, NCT04711850</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2024-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15383","citationCount":"0","resultStr":"{\"title\":\"A Randomized Trial Comparing Imlifidase to Plasmapheresis in Kidney Transplant Recipients With Antibody-Mediated Rejection\",\"authors\":\"Fabian Halleck, Georg A. Böhmig, Lionel Couzi, Lionel Rostaing, Gunilla Einecke, Carmen Lefaucheur, Christophe Legendre, Robert Montgomery, Peter Hughes, Anil Chandraker, Kate Wyburn, Phil Halloran, Angela Q. Maldonado, Kristoffer Sjöholm, Anna Runström, Paola Lefèvre, Jan Tollemar, Stanley Jordan\",\"doi\":\"10.1111/ctr.15383\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Antibody-mediated rejection (ABMR) poses a barrier to long-term graft survival and is one of the most challenging events after kidney transplantation. Removing donor specific antibodies (DSA) through therapeutic plasma exchange (PLEX) is a cornerstone of antibody depletion but has inconsistent effects. Imlifidase is a treatment currently utilized for desensitization with near-complete inactivation of DSA both in the intra- and extravascular space.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a 6-month, randomized, open-label, multicenter, multinational trial conducted at 14 transplant centers. Thirty patients were randomized to either imlifidase or PLEX treatment. The primary endpoint was reduction in DSA level during the 5 days following the start of treatment.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Despite considerable heterogeneity in the trial population, DSA reduction as defined by the primary endpoint was 97% for imlifidase compared to 42% for PLEX. Additionally, imlifidase reduced DSA to noncomplement fixing levels, whereas PLEX failed to do so. After antibody rebound in the imlifidase arm (circa days 6–12), both arms had similar reductions in DSA. Five allograft losses occurred during the 6 months following the start of ABMR treatment—four within the imlifidase arm (18 patients treated) and one in the PLEX arm (10 patients treated). In terms of clinical efficacy, the Kaplan–Meier estimated graft survival was 78% for imlifidase and 89% for PLEX, with a slightly higher eGFR in the PLEX arm at the end of the trial. The observed adverse events in the trial were as expected, and there were no apparent differences between the arms.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Imlifidase was safe and well-tolerated in the ABMR population. Despite meeting the primary endpoint of maximum DSA reduction compared to PLEX, the trial was unsuccessful in demonstrating a clinical benefit of imlifidase in this heterogenous ABMR population.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Trial Registration</h3>\\n \\n <p>EudraCT number: 2018-000022-66, 2020-004777-49; ClinicalTrials.gov identifier: NCT03897205, NCT04711850</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15383\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15383\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15383","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
A Randomized Trial Comparing Imlifidase to Plasmapheresis in Kidney Transplant Recipients With Antibody-Mediated Rejection
Background
Antibody-mediated rejection (ABMR) poses a barrier to long-term graft survival and is one of the most challenging events after kidney transplantation. Removing donor specific antibodies (DSA) through therapeutic plasma exchange (PLEX) is a cornerstone of antibody depletion but has inconsistent effects. Imlifidase is a treatment currently utilized for desensitization with near-complete inactivation of DSA both in the intra- and extravascular space.
Methods
This was a 6-month, randomized, open-label, multicenter, multinational trial conducted at 14 transplant centers. Thirty patients were randomized to either imlifidase or PLEX treatment. The primary endpoint was reduction in DSA level during the 5 days following the start of treatment.
Results
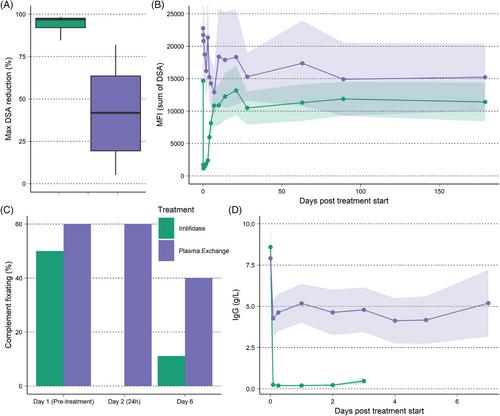
Despite considerable heterogeneity in the trial population, DSA reduction as defined by the primary endpoint was 97% for imlifidase compared to 42% for PLEX. Additionally, imlifidase reduced DSA to noncomplement fixing levels, whereas PLEX failed to do so. After antibody rebound in the imlifidase arm (circa days 6–12), both arms had similar reductions in DSA. Five allograft losses occurred during the 6 months following the start of ABMR treatment—four within the imlifidase arm (18 patients treated) and one in the PLEX arm (10 patients treated). In terms of clinical efficacy, the Kaplan–Meier estimated graft survival was 78% for imlifidase and 89% for PLEX, with a slightly higher eGFR in the PLEX arm at the end of the trial. The observed adverse events in the trial were as expected, and there were no apparent differences between the arms.
Conclusion
Imlifidase was safe and well-tolerated in the ABMR population. Despite meeting the primary endpoint of maximum DSA reduction compared to PLEX, the trial was unsuccessful in demonstrating a clinical benefit of imlifidase in this heterogenous ABMR population.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


