Salmir Nasic, Johan Mölne, Marie Eriksson, Bernd Stegmayr, Henri Afghahi, Björn Peters
{"title":"两次连续活检之间肾小球巨噬细胞数量的变化及其与肾移植移植物存活率的关系","authors":"Salmir Nasic, Johan Mölne, Marie Eriksson, Bernd Stegmayr, Henri Afghahi, Björn Peters","doi":"10.1111/ctr.15384","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Macrophages are involved in kidney transplants. The aim of the study was to investigate if changes exist in the levels of glomerular macrophage index (GMI) between two consecutive kidney transplant biopsies, and if so to determine their potential impact on graft survival.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Two consecutive biopsies were performed on the same renal graft in 623 patients. GMI was categorized into three GMI classes: ≤1.8 Low, 1.9–4.5 Medium, and ≥4.6 High. This division yielded nine possible switches between the first and second biopsies (Low-Low, Low-Medium, etc.). Cox-regressions were used and hazard ratios (HR) with 95% confidence interval (CI) are presented.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The worst graft survival was observed in the High-High group, and the best graft survival was observed in the Low-Low and High-Low groups. Compared to the High-High group, a reduction of risk was observed in nearly all other decreasing groups (reductions between 65% and 80% of graft loss). After adjustment for covariates, the risk for graft-loss was lower in the Low-Low (HR = 0.24, CI 0.13–0.46), Low-Medium (HR = 0.25, CI 0.11–0.55), Medium-Low (HR = 0.29, CI 0.11–0.77), and the High-Low GMI (HR = 0.31, CI 0.10–0.98) groups compared to the High-High group as the reference.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>GMI may change dynamically, and the latest finding is of most prognostic importance. GMI should be considered in all evaluations of biopsy findings since high or increasing GMI levels are associated with shorter graft survival. Future studies need to consider therapeutic strategies to lower or maintain a low GMI. A high GMI besides a vague histological finding should be considered as a warning sign requiring more frequent clinical follow up.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2024-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15384","citationCount":"0","resultStr":"{\"title\":\"Changes in Numbers of Glomerular Macrophages Between Two Consecutive Biopsies and the Association With Renal Transplant Graft Survival\",\"authors\":\"Salmir Nasic, Johan Mölne, Marie Eriksson, Bernd Stegmayr, Henri Afghahi, Björn Peters\",\"doi\":\"10.1111/ctr.15384\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Macrophages are involved in kidney transplants. The aim of the study was to investigate if changes exist in the levels of glomerular macrophage index (GMI) between two consecutive kidney transplant biopsies, and if so to determine their potential impact on graft survival.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Two consecutive biopsies were performed on the same renal graft in 623 patients. GMI was categorized into three GMI classes: ≤1.8 Low, 1.9–4.5 Medium, and ≥4.6 High. This division yielded nine possible switches between the first and second biopsies (Low-Low, Low-Medium, etc.). Cox-regressions were used and hazard ratios (HR) with 95% confidence interval (CI) are presented.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The worst graft survival was observed in the High-High group, and the best graft survival was observed in the Low-Low and High-Low groups. Compared to the High-High group, a reduction of risk was observed in nearly all other decreasing groups (reductions between 65% and 80% of graft loss). After adjustment for covariates, the risk for graft-loss was lower in the Low-Low (HR = 0.24, CI 0.13–0.46), Low-Medium (HR = 0.25, CI 0.11–0.55), Medium-Low (HR = 0.29, CI 0.11–0.77), and the High-Low GMI (HR = 0.31, CI 0.10–0.98) groups compared to the High-High group as the reference.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>GMI may change dynamically, and the latest finding is of most prognostic importance. GMI should be considered in all evaluations of biopsy findings since high or increasing GMI levels are associated with shorter graft survival. Future studies need to consider therapeutic strategies to lower or maintain a low GMI. A high GMI besides a vague histological finding should be considered as a warning sign requiring more frequent clinical follow up.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-07-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15384\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15384\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15384","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Changes in Numbers of Glomerular Macrophages Between Two Consecutive Biopsies and the Association With Renal Transplant Graft Survival
Background
Macrophages are involved in kidney transplants. The aim of the study was to investigate if changes exist in the levels of glomerular macrophage index (GMI) between two consecutive kidney transplant biopsies, and if so to determine their potential impact on graft survival.
Methods
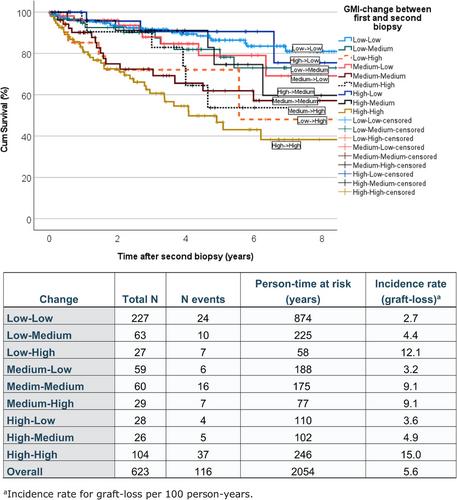
Two consecutive biopsies were performed on the same renal graft in 623 patients. GMI was categorized into three GMI classes: ≤1.8 Low, 1.9–4.5 Medium, and ≥4.6 High. This division yielded nine possible switches between the first and second biopsies (Low-Low, Low-Medium, etc.). Cox-regressions were used and hazard ratios (HR) with 95% confidence interval (CI) are presented.
Results
The worst graft survival was observed in the High-High group, and the best graft survival was observed in the Low-Low and High-Low groups. Compared to the High-High group, a reduction of risk was observed in nearly all other decreasing groups (reductions between 65% and 80% of graft loss). After adjustment for covariates, the risk for graft-loss was lower in the Low-Low (HR = 0.24, CI 0.13–0.46), Low-Medium (HR = 0.25, CI 0.11–0.55), Medium-Low (HR = 0.29, CI 0.11–0.77), and the High-Low GMI (HR = 0.31, CI 0.10–0.98) groups compared to the High-High group as the reference.
Conclusions
GMI may change dynamically, and the latest finding is of most prognostic importance. GMI should be considered in all evaluations of biopsy findings since high or increasing GMI levels are associated with shorter graft survival. Future studies need to consider therapeutic strategies to lower or maintain a low GMI. A high GMI besides a vague histological finding should be considered as a warning sign requiring more frequent clinical follow up.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


