Madelyn Agaciak, Molla M Wassie, Kalindra Simpson, Charles Cock, Peter Bampton, Robert Fraser, Erin L Symonds
{"title":"75 岁以上无症状参与者的结肠镜监测结果","authors":"Madelyn Agaciak, Molla M Wassie, Kalindra Simpson, Charles Cock, Peter Bampton, Robert Fraser, Erin L Symonds","doi":"10.1002/jgh3.13071","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aim</h3>\n \n <p>Surveillance colonoscopy for colorectal cancer (CRC) is generally not recommended beyond 75 years of age. The study determined incidence and predictors of advanced adenoma and CRC in older individuals undergoing surveillance colonoscopy.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a retrospective cohort study of asymptomatic older participants (≥75 years), enrolled in a South Australian CRC surveillance program who underwent colonoscopy (2015–2020). Clinical records were extracted for demographics, personal or family history of CRC, comorbidities, polypharmacy, and colonoscopy findings. The associations between clinical variables and advanced adenoma or CRC at surveillance were assessed with multivariable Poisson regression analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Totally 698 surveillance colonoscopies were analyzed from 574 participants aged 75–91 years (55.6% male). The incidence of CRC was 1.6% (11/698), while 37.9% (260/698) of procedures had advanced adenoma detected. Previous CRC (incidence rate ratio [IRR] 5.9, 95% CI 1.5–22.5), age ≥85 years (IRR 5.8, 95% CI 1.6–20.1) and active smoking (IRR 4.9, 95% CI 1.0–24.4) were independently associated with CRC diagnosis, while advanced adenoma at immediately preceding colonoscopy (IRR 1.6, 95% CI 1.3–2.0) and polypharmacy (IRR 1.2, 95% CI 1.0–1.5) were associated with advanced adenoma at surveillance colonoscopy in asymptomatic older participants (≥75 years).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Advanced neoplasia was found in more than one third of the surveillance procedures completed in this cohort. Continuation of surveillance beyond age 75 yeasrs may be considered in participants who have previous CRC or are active smokers (provided they are fit to undergo colonoscopy). In other cases, such as past advanced adenoma only, the need for ongoing surveillance should be considered alongside participant preference and health status.</p>\n </section>\n </div>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 5","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.13071","citationCount":"0","resultStr":"{\"title\":\"Surveillance colonoscopy findings in asymptomatic participants over 75 years of age\",\"authors\":\"Madelyn Agaciak, Molla M Wassie, Kalindra Simpson, Charles Cock, Peter Bampton, Robert Fraser, Erin L Symonds\",\"doi\":\"10.1002/jgh3.13071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background and Aim</h3>\\n \\n <p>Surveillance colonoscopy for colorectal cancer (CRC) is generally not recommended beyond 75 years of age. The study determined incidence and predictors of advanced adenoma and CRC in older individuals undergoing surveillance colonoscopy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a retrospective cohort study of asymptomatic older participants (≥75 years), enrolled in a South Australian CRC surveillance program who underwent colonoscopy (2015–2020). Clinical records were extracted for demographics, personal or family history of CRC, comorbidities, polypharmacy, and colonoscopy findings. The associations between clinical variables and advanced adenoma or CRC at surveillance were assessed with multivariable Poisson regression analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Totally 698 surveillance colonoscopies were analyzed from 574 participants aged 75–91 years (55.6% male). The incidence of CRC was 1.6% (11/698), while 37.9% (260/698) of procedures had advanced adenoma detected. Previous CRC (incidence rate ratio [IRR] 5.9, 95% CI 1.5–22.5), age ≥85 years (IRR 5.8, 95% CI 1.6–20.1) and active smoking (IRR 4.9, 95% CI 1.0–24.4) were independently associated with CRC diagnosis, while advanced adenoma at immediately preceding colonoscopy (IRR 1.6, 95% CI 1.3–2.0) and polypharmacy (IRR 1.2, 95% CI 1.0–1.5) were associated with advanced adenoma at surveillance colonoscopy in asymptomatic older participants (≥75 years).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Advanced neoplasia was found in more than one third of the surveillance procedures completed in this cohort. Continuation of surveillance beyond age 75 yeasrs may be considered in participants who have previous CRC or are active smokers (provided they are fit to undergo colonoscopy). In other cases, such as past advanced adenoma only, the need for ongoing surveillance should be considered alongside participant preference and health status.</p>\\n </section>\\n </div>\",\"PeriodicalId\":45861,\"journal\":{\"name\":\"JGH Open\",\"volume\":\"8 5\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.13071\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JGH Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Surveillance colonoscopy findings in asymptomatic participants over 75 years of age
Background and Aim
Surveillance colonoscopy for colorectal cancer (CRC) is generally not recommended beyond 75 years of age. The study determined incidence and predictors of advanced adenoma and CRC in older individuals undergoing surveillance colonoscopy.
Methods
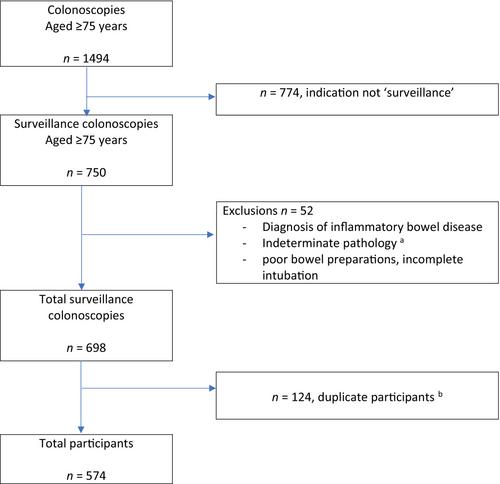
This was a retrospective cohort study of asymptomatic older participants (≥75 years), enrolled in a South Australian CRC surveillance program who underwent colonoscopy (2015–2020). Clinical records were extracted for demographics, personal or family history of CRC, comorbidities, polypharmacy, and colonoscopy findings. The associations between clinical variables and advanced adenoma or CRC at surveillance were assessed with multivariable Poisson regression analysis.
Results
Totally 698 surveillance colonoscopies were analyzed from 574 participants aged 75–91 years (55.6% male). The incidence of CRC was 1.6% (11/698), while 37.9% (260/698) of procedures had advanced adenoma detected. Previous CRC (incidence rate ratio [IRR] 5.9, 95% CI 1.5–22.5), age ≥85 years (IRR 5.8, 95% CI 1.6–20.1) and active smoking (IRR 4.9, 95% CI 1.0–24.4) were independently associated with CRC diagnosis, while advanced adenoma at immediately preceding colonoscopy (IRR 1.6, 95% CI 1.3–2.0) and polypharmacy (IRR 1.2, 95% CI 1.0–1.5) were associated with advanced adenoma at surveillance colonoscopy in asymptomatic older participants (≥75 years).
Conclusion
Advanced neoplasia was found in more than one third of the surveillance procedures completed in this cohort. Continuation of surveillance beyond age 75 yeasrs may be considered in participants who have previous CRC or are active smokers (provided they are fit to undergo colonoscopy). In other cases, such as past advanced adenoma only, the need for ongoing surveillance should be considered alongside participant preference and health status.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


