{"title":"Factors Affecting Survival and Local Control in Patients with Bone Metastases Treated with Radiotherapy.","authors":"Kenji Makita, Yasushi Hamamoto, Hiromitsu Kanzaki, Kei Nagasaki, Noriko Takata, Shintaro Tsuruoka, Kotaro Uwatsu, Teruhito Kido","doi":"10.3390/medsci11010017","DOIUrl":null,"url":null,"abstract":"<p><p>The aim of this study was to evaluate the expected prognosis and factors affecting local control (LC) of the bone metastatic sites treated with palliative external beam radiotherapy (RT). Between December 2010 and April 2019, 420 cases (male/female = 240/180; median age [range]: 66 [12-90] years) with predominantly osteolytic bone metastases received RT and were evaluated. LC was evaluated by follow-up computed tomography (CT) image. Median RT doses (BED<sub>10</sub>) were 39.0 Gy (range, 14.4-71.7 Gy). The 0.5-year overall survival and LC of RT sites were 71% and 84%, respectively. Local recurrence on CT images was observed in 19% (<i>n</i> = 80) of the RT sites, and the median recurrence time was 3.5 months (range, 1-106 months). In univariate analysis, abnormal laboratory data before RT (platelet count, serum albumin, total bilirubin, lactate dehydrogenase, or serum calcium level), high-risk primary tumor sites (colorectal, esophageal, hepatobiliary/pancreatic, renal/ureter, and non-epithelial cancers), no antineoplastic agents (ATs) administration after RT, and no bone modifying agents (BMAs) administration after RT were significantly unfavorable factors for both survival and LC of RT sites. Sex (male), performance status (≥3), and RT dose (BED<sub>10</sub>) (<39.0 Gy) were significantly unfavorable factors for only survival, and age (≥70 years) and bone cortex destruction were significantly unfavorable factors for only LC of RT sites. In multivariate analysis, only abnormal laboratory data before RT influenced both unfavorable survival and LC of RT sites. Performance status (≥3), no ATs administration after RT, RT dose (BED<sub>10</sub>) (<39.0 Gy), and sex (male) were significantly unfavorable factors for survival, and primary tumor sites and BMAs administration after RT were significantly unfavorable factors for LC of RT sites. In conclusion, laboratory data before RT was important factor both prognosis and LC of bone metastases treated with palliative RT. At least in patients with abnormal laboratory data before RT, palliative RT seemed to be focused on the only pain relief.</p>","PeriodicalId":74152,"journal":{"name":"Medical sciences (Basel, Switzerland)","volume":"11 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9944514/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical sciences (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medsci11010017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
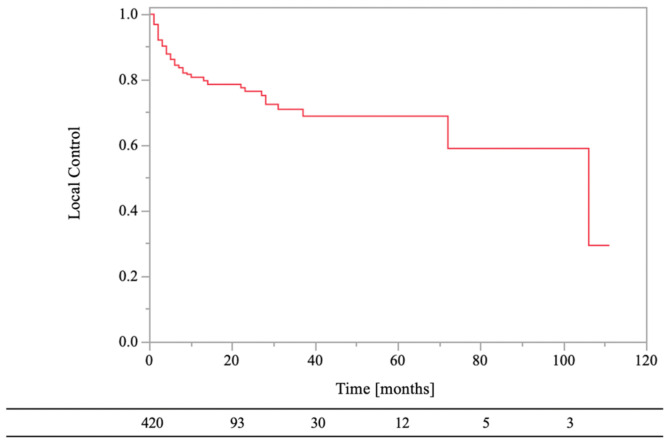
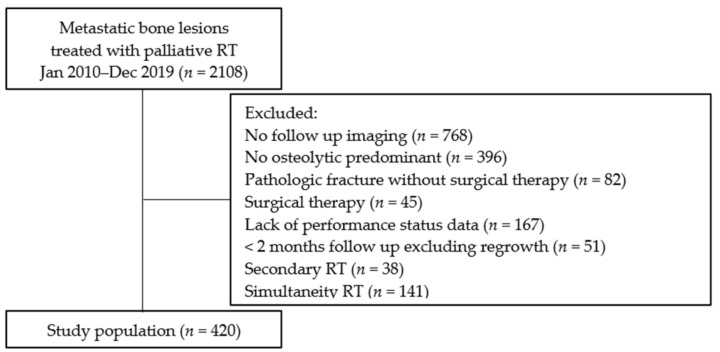
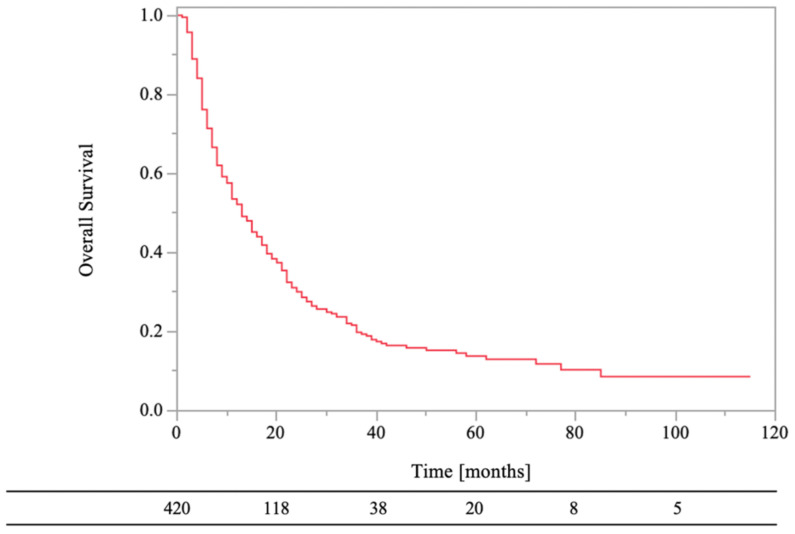
The aim of this study was to evaluate the expected prognosis and factors affecting local control (LC) of the bone metastatic sites treated with palliative external beam radiotherapy (RT). Between December 2010 and April 2019, 420 cases (male/female = 240/180; median age [range]: 66 [12-90] years) with predominantly osteolytic bone metastases received RT and were evaluated. LC was evaluated by follow-up computed tomography (CT) image. Median RT doses (BED10) were 39.0 Gy (range, 14.4-71.7 Gy). The 0.5-year overall survival and LC of RT sites were 71% and 84%, respectively. Local recurrence on CT images was observed in 19% (n = 80) of the RT sites, and the median recurrence time was 3.5 months (range, 1-106 months). In univariate analysis, abnormal laboratory data before RT (platelet count, serum albumin, total bilirubin, lactate dehydrogenase, or serum calcium level), high-risk primary tumor sites (colorectal, esophageal, hepatobiliary/pancreatic, renal/ureter, and non-epithelial cancers), no antineoplastic agents (ATs) administration after RT, and no bone modifying agents (BMAs) administration after RT were significantly unfavorable factors for both survival and LC of RT sites. Sex (male), performance status (≥3), and RT dose (BED10) (<39.0 Gy) were significantly unfavorable factors for only survival, and age (≥70 years) and bone cortex destruction were significantly unfavorable factors for only LC of RT sites. In multivariate analysis, only abnormal laboratory data before RT influenced both unfavorable survival and LC of RT sites. Performance status (≥3), no ATs administration after RT, RT dose (BED10) (<39.0 Gy), and sex (male) were significantly unfavorable factors for survival, and primary tumor sites and BMAs administration after RT were significantly unfavorable factors for LC of RT sites. In conclusion, laboratory data before RT was important factor both prognosis and LC of bone metastases treated with palliative RT. At least in patients with abnormal laboratory data before RT, palliative RT seemed to be focused on the only pain relief.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


