Mitsouko van Assche, Elisabeth Dirren, Alexia Bourgeois, Andreas Kleinschmidt, Jonas Richiardi, Emmanuel Carrera
{"title":"Periinfarct rewiring supports recovery after primary motor cortex stroke.","authors":"Mitsouko van Assche, Elisabeth Dirren, Alexia Bourgeois, Andreas Kleinschmidt, Jonas Richiardi, Emmanuel Carrera","doi":"10.1177/0271678X211002968","DOIUrl":null,"url":null,"abstract":"<p><p>After stroke restricted to the primary motor cortex (M1), it is uncertain whether network reorganization associated with recovery involves the periinfarct or more remote regions. We studied 16 patients with focal M1 stroke and hand paresis. Motor function and resting-state MRI functional connectivity (FC) were assessed at three time points: acute (<10 days), early subacute (3 weeks), and late subacute (3 months). FC correlates of recovery were investigated at three spatial scales, (i) ipsilesional non-infarcted M1, (ii) core motor network (M1, premotor cortex (PMC), supplementary motor area (SMA), and primary somatosensory cortex), and (iii) extended motor network including all regions structurally connected to the upper limb representation of M1. Hand dexterity was impaired only in the acute phase (<i>P</i> = 0.036). At a small spatial scale, clinical recovery was more frequently associated with connections involving ipsilesional non-infarcted M1 (Odds Ratio = 6.29; <i>P =</i> 0.036). At a larger scale, recovery correlated with increased FC strength in the core network compared to the extended motor network (rho = 0.71;<i>P</i> = 0.006). These results suggest that FC changes associated with motor improvement involve the perilesional M1 and do not extend beyond the core motor network. Core motor regions, and more specifically ipsilesional non-infarcted M1, could hence become primary targets for restorative therapies.</p>","PeriodicalId":520660,"journal":{"name":"Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism","volume":" ","pages":"2174-2184"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/0271678X211002968","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/0271678X211002968","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/3/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
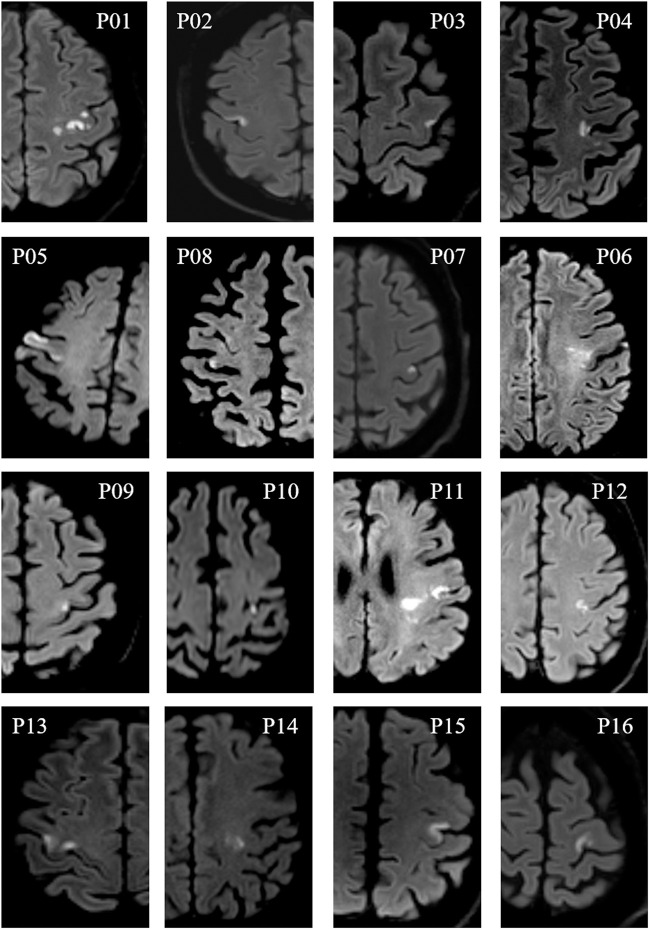
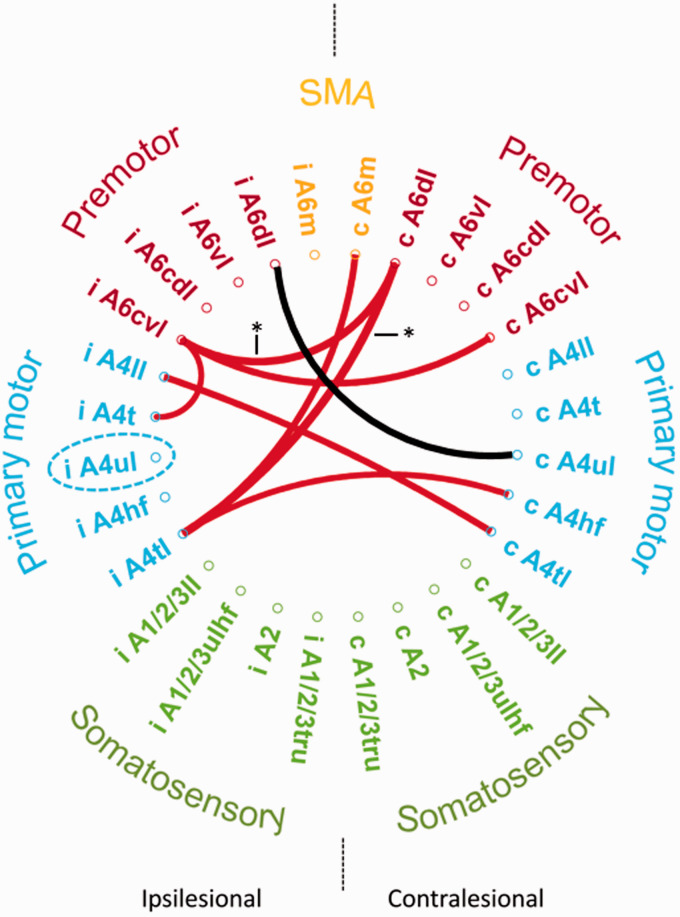
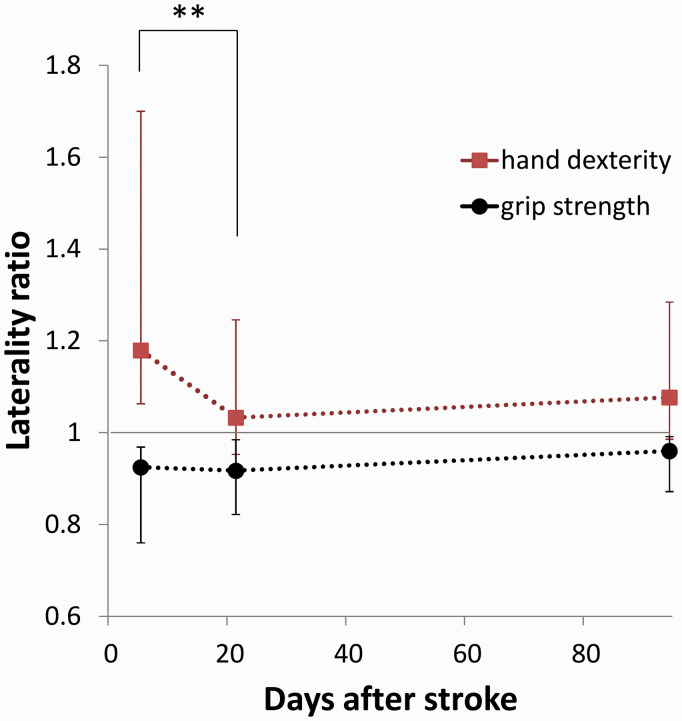
After stroke restricted to the primary motor cortex (M1), it is uncertain whether network reorganization associated with recovery involves the periinfarct or more remote regions. We studied 16 patients with focal M1 stroke and hand paresis. Motor function and resting-state MRI functional connectivity (FC) were assessed at three time points: acute (<10 days), early subacute (3 weeks), and late subacute (3 months). FC correlates of recovery were investigated at three spatial scales, (i) ipsilesional non-infarcted M1, (ii) core motor network (M1, premotor cortex (PMC), supplementary motor area (SMA), and primary somatosensory cortex), and (iii) extended motor network including all regions structurally connected to the upper limb representation of M1. Hand dexterity was impaired only in the acute phase (P = 0.036). At a small spatial scale, clinical recovery was more frequently associated with connections involving ipsilesional non-infarcted M1 (Odds Ratio = 6.29; P = 0.036). At a larger scale, recovery correlated with increased FC strength in the core network compared to the extended motor network (rho = 0.71;P = 0.006). These results suggest that FC changes associated with motor improvement involve the perilesional M1 and do not extend beyond the core motor network. Core motor regions, and more specifically ipsilesional non-infarcted M1, could hence become primary targets for restorative therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


