Roaa Shoukry, Alexandra Moskalewicz, Nicole Bradley, Elizabeth Bond, Mandy Sala, Sumit Gupta, Paul Gibson, Petros Pechlivanoglou
{"title":"Cost–utility of nelarabine for the first-line treatment of newly diagnosed pediatric T-cell acute lymphoblastic leukemia in Canada","authors":"Roaa Shoukry, Alexandra Moskalewicz, Nicole Bradley, Elizabeth Bond, Mandy Sala, Sumit Gupta, Paul Gibson, Petros Pechlivanoglou","doi":"10.1002/pbc.31393","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The Children's Oncology Group (COG)-AALL0434 trial investigated the addition of nelarabine to the augmented Berlin–Frankfurt–Münster (aBFM) protocol in patients (1.0–30.99 years) with newly diagnosed T-cell acute lymphoblastic leukemia (T-ALL). Despite demonstrating superior outcomes, nelarabine is not currently funded by many health systems, in part due to a lack of cost-effectiveness data. We estimated the cost–utility of nelarabine for this indication from a Canadian public healthcare payer perspective.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We developed a microsimulation model that followed hypothetical patients with newly diagnosed T-ALL from post-induction therapy to death. Three health states were modeled: relapse-free, post-relapse, and death. Efficacy was estimated using AALL0434 and retrospective data from Ontario, Canada. Costs were obtained from Canadian sources. Utility estimates and long-term mortality risks were sourced from literature. Total healthcare costs, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER) were reported. Probabilistic and scenario analyses were conducted.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Incorporating nelarabine in the aBFM protocol increased costs by $51,670 Canadian dollars per patient, but resulted in 1.97 more QALYs and an ICER of $26,184/QALY. Most of the identified cost and benefit were accrued within the AALL0434 trial period (first 11 years post diagnosis) and while patients were in the relapse-free health state. Across multiple scenarios, the ICER was stable under an assumed $50,000/QALY threshold.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Incorporating nelarabine into aBFM was cost-effective across different scenarios and assumptions. These results support its funding by public and private payers.</p>\n </section>\n </div>","PeriodicalId":19822,"journal":{"name":"Pediatric Blood & Cancer","volume":"72 1","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-10-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/pbc.31393","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Blood & Cancer","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/pbc.31393","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The Children's Oncology Group (COG)-AALL0434 trial investigated the addition of nelarabine to the augmented Berlin–Frankfurt–Münster (aBFM) protocol in patients (1.0–30.99 years) with newly diagnosed T-cell acute lymphoblastic leukemia (T-ALL). Despite demonstrating superior outcomes, nelarabine is not currently funded by many health systems, in part due to a lack of cost-effectiveness data. We estimated the cost–utility of nelarabine for this indication from a Canadian public healthcare payer perspective.
Methods
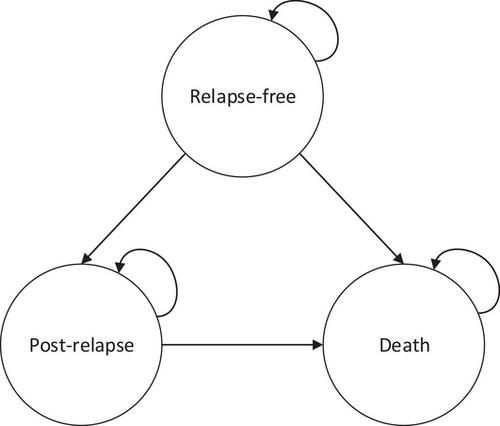
We developed a microsimulation model that followed hypothetical patients with newly diagnosed T-ALL from post-induction therapy to death. Three health states were modeled: relapse-free, post-relapse, and death. Efficacy was estimated using AALL0434 and retrospective data from Ontario, Canada. Costs were obtained from Canadian sources. Utility estimates and long-term mortality risks were sourced from literature. Total healthcare costs, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER) were reported. Probabilistic and scenario analyses were conducted.
Results
Incorporating nelarabine in the aBFM protocol increased costs by $51,670 Canadian dollars per patient, but resulted in 1.97 more QALYs and an ICER of $26,184/QALY. Most of the identified cost and benefit were accrued within the AALL0434 trial period (first 11 years post diagnosis) and while patients were in the relapse-free health state. Across multiple scenarios, the ICER was stable under an assumed $50,000/QALY threshold.
Conclusion
Incorporating nelarabine into aBFM was cost-effective across different scenarios and assumptions. These results support its funding by public and private payers.
期刊介绍:
Pediatric Blood & Cancer publishes the highest quality manuscripts describing basic and clinical investigations of blood disorders and malignant diseases of childhood including diagnosis, treatment, epidemiology, etiology, biology, and molecular and clinical genetics of these diseases as they affect children, adolescents, and young adults. Pediatric Blood & Cancer will also include studies on such treatment options as hematopoietic stem cell transplantation, immunology, and gene therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


