Malnutrition in emergency general surgery: a survey of National Emergency Laparotomy Audit Leads
Abstract
Background
Patients who are malnourished and have emergency general surgery, such as a laparotomy, have worse outcomes than those who are not malnourished. It is paramount to identify these patients and minimise this risk. This study aimed to describe current practices in identifying malnutrition in patients undergoing a laparotomy, specifically focusing on screening, assessment, nutrition pathways and barriers encountered by clinicians.
Methods
Following piloting and validity assessment, anaesthetic and surgical National Emergency Laparotomy Audit (NELA) Leads at hospitals across England and Wales were emailed an invitation to a survey. Responses were gathered using Qualtrics. Descriptive analysis and correlation with laparotomy volume and professional role were performed in SPSSv26. University of Sheffield ethical approval was obtained (UREC 046205). The results from the survey are reported according to the CHERRIES guidelines.
Results
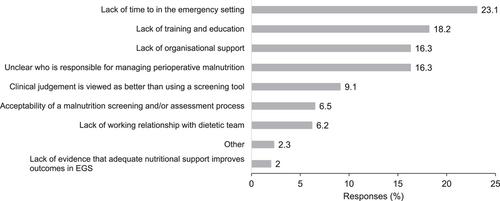
The survey was completed by 166/289 NELA Leads from 117/167 hospitals (57.4% and 70.1% response rates, respectively). Participants reported low rates of nutritional screening (42/166; 25.3%) and assessment (26/166; 15.7%) for malnutrition preoperatively. More than one third of respondents (40.1%) had no awareness of local screening tools; indeed, the Malnutrition Universal Screening Tool (MUST) was used by approximately half of respondents (56.6%). Contrary to guidelines, NELA Leads report albumin levels continue to be used to determine malnutrition risk (73.5%; 122/166). Postoperative nutrition pathways were common (71.7%; 119/166). Reported barriers to nutritional screening and assessment included a lack of time, training and education, organisational support and ownership. Participants indicated nutrition risk is inadequately identified and is an important missing data item from NELA. There was no significant correlation with hospital laparotomy volume in relation to screening or assessment for malnutrition, the use of nutritional support pathways or organisational barriers. There was interprofessional agreement across a number of domains, although some differences did exist.
Conclusions
Wide variation exists in the current practice of identifying malnutrition risk in NELA patients. Barriers include a lack of time, knowledge and ownership. Nutrition pathways that encompass the preoperative phase and incorporation of nutrition data in NELA may support improvements in care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


