Jee-Heon Kim MD, Young-Chae Yoon MD, Young-Hoon Kim MD, Jong-Il Park MD, Kang-Un Choi MD, Jong-Ho Nam MD, Chan-Hee Lee MD, Jang-Won Son MD, Jong-Seon Park MD, Ung Kim MD, PhD
{"title":"Cardiovascular outcomes between dapagliflozin versus empagliflozin in patients with diabetes mellitus","authors":"Jee-Heon Kim MD, Young-Chae Yoon MD, Young-Hoon Kim MD, Jong-Il Park MD, Kang-Un Choi MD, Jong-Ho Nam MD, Chan-Hee Lee MD, Jang-Won Son MD, Jong-Seon Park MD, Ung Kim MD, PhD","doi":"10.1002/clc.24248","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Sodium-glucose co-transporter 2 (SGLT2) inhibitors have been demonstrated to decrease cardiovascular adverse events. However, there is little real-world clinical evidence regarding a direct comparison between dapagliflozin and empagliflozin in patients with diabetes mellitus (DM).</p>\n </section>\n \n <section>\n \n <h3> Hypothesis</h3>\n \n <p>A difference in the cardiovascular efficancy of dapagliflozin versus empagliflozin in DM patients was anticipated, aiming to guide the optimal choice of SGLT2 inhibitors based on cardiovascular outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>From 2014 to 2020, a total of 1549 patients with DM who were prescribed SGLT2 inhibitors such as dapagliflozin or empagliflozin were retrospectively enrolled. We categorized the study population into two groups: dapagliflozin (<i>n</i> = 981) and empagliflozin group (<i>n</i> = 568). The primary endpoint was major adverse cardiovascular events (MACE), defined as a composite of all-cause death, myocardial infarction (MI), stroke, or hospitalization for heart failure (HF) over a 3-year period.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Propensity-score matching was performed (537 patients in each group). The mean age and hemoglobin A1c were 58.2 ± 13.0 years and 8.4 ± 1.7%, respectively. There was no significant difference between the dapagliflozin and empagliflozin groups in the risk of MACE (3.7% vs. 4.8%, hazard ratio [HR], 1.31; 95% confidence interval [CI], 0.73–2.35; <i>p</i> = 0.349). Furthermore, there were no differences between the two groups in secondary endpoints including all-cause death, MI, stroke, and hospitalization for HF. Prior MI and history of HF were independent predictors of MACE.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Dapagliflozin and empagliflozin showed no significant difference of real-world clinical cardiovascular outcomes in patients with DM over a 3-year period. Further large randomized clinical trials will be warranted for better evaluation.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":null,"pages":null},"PeriodicalIF":2.4000,"publicationDate":"2024-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24248","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24248","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Sodium-glucose co-transporter 2 (SGLT2) inhibitors have been demonstrated to decrease cardiovascular adverse events. However, there is little real-world clinical evidence regarding a direct comparison between dapagliflozin and empagliflozin in patients with diabetes mellitus (DM).
Hypothesis
A difference in the cardiovascular efficancy of dapagliflozin versus empagliflozin in DM patients was anticipated, aiming to guide the optimal choice of SGLT2 inhibitors based on cardiovascular outcomes.
Methods
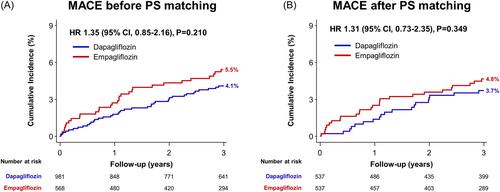
From 2014 to 2020, a total of 1549 patients with DM who were prescribed SGLT2 inhibitors such as dapagliflozin or empagliflozin were retrospectively enrolled. We categorized the study population into two groups: dapagliflozin (n = 981) and empagliflozin group (n = 568). The primary endpoint was major adverse cardiovascular events (MACE), defined as a composite of all-cause death, myocardial infarction (MI), stroke, or hospitalization for heart failure (HF) over a 3-year period.
Results
Propensity-score matching was performed (537 patients in each group). The mean age and hemoglobin A1c were 58.2 ± 13.0 years and 8.4 ± 1.7%, respectively. There was no significant difference between the dapagliflozin and empagliflozin groups in the risk of MACE (3.7% vs. 4.8%, hazard ratio [HR], 1.31; 95% confidence interval [CI], 0.73–2.35; p = 0.349). Furthermore, there were no differences between the two groups in secondary endpoints including all-cause death, MI, stroke, and hospitalization for HF. Prior MI and history of HF were independent predictors of MACE.
Conclusions
Dapagliflozin and empagliflozin showed no significant difference of real-world clinical cardiovascular outcomes in patients with DM over a 3-year period. Further large randomized clinical trials will be warranted for better evaluation.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


