Does Collaboration between General Practitioners and Pharmacists Improve Risk Factors for Cardiovascular Disease and Diabetes? A Systematic Review and Meta-Analysis.
Kanika Chaudhri, Gabriella Caleres, Samantha Saunders, Peter Michail, Gian Luca Di Tanna, Thomas Lung, Hueiming Liu, Rohina Joshi
{"title":"Does Collaboration between General Practitioners and Pharmacists Improve Risk Factors for Cardiovascular Disease and Diabetes? A Systematic Review and Meta-Analysis.","authors":"Kanika Chaudhri, Gabriella Caleres, Samantha Saunders, Peter Michail, Gian Luca Di Tanna, Thomas Lung, Hueiming Liu, Rohina Joshi","doi":"10.5334/gh.1184","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess whether inter-professional, bidirectional collaboration between general practitioners (GPs) and pharmacists has an impact on improving cardiovascular risk outcomes among patients in the primary care setting. It also aimed to understand the different types of collaborative care models used.</p><p><strong>Study design: </strong>Systematic review and Hartung-Knapp-Sidik-Jonkman random effects meta-analyses of randomised control trials (RCTs) in inter-professional bidirectional collaboration between GP and pharmacists assessing a change of patient cardiovascular risk in the primary care setting.</p><p><strong>Data sources: </strong>MEDLINE, EMBASE, Cochrane, CINAHL and International Pharmaceutical Abstracts, scanned reference lists of relevant studies, hand searched key journals and key papers until August 2021.</p><p><strong>Data synthesis: </strong>Twenty-eight RCTs were identified. Collaboration was associated with significant reductions in systolic and diastolic blood pressure (23 studies, 5,620 participants) of -6.42 mmHg (95% confidence interval (95%CI) -7.99 to -4.84) and -2.33 mmHg (95%CI -3.76 to -0.91), respectively. Changes in other cardiovascular risk factors included total cholesterol (6 studies, 1,917 participants) -0.26 mmol/L (95%CI -0.49 to -0.03); low-density lipoprotein (8 studies, 1,817 participants) -0.16 mmol/L (95%CI -0.63 to 0.32); high-density lipoprotein (7 studies, 1,525 participants) 0.02 mmol/L (95%CI -0.02 to 0.07). Reduction in haemoglobin A1c (HbA1C) (10 studies, 2,025 participants), body mass index (8 studies, 1,708 participants) and smoking cessation (1 study, 132 participants) was observed with GP-pharmacist collaboration. Meta-analysis was not conducted for these changes. Various models of collaborative care included verbal communication (via phone calls or face to face), and written communication (emails, letters). We found that co-location was associated with positive changes in cardiovascular risk factors.</p><p><strong>Conclusion: </strong>Although it is clear that collaborative care is ideal compared to usual care, greater details in the description of the collaborative model of care in studies is required for a core comprehensive evaluation of the different models of collaboration.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"18 1","pages":"7"},"PeriodicalIF":3.0000,"publicationDate":"2023-02-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9951619/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1184","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To assess whether inter-professional, bidirectional collaboration between general practitioners (GPs) and pharmacists has an impact on improving cardiovascular risk outcomes among patients in the primary care setting. It also aimed to understand the different types of collaborative care models used.
Study design: Systematic review and Hartung-Knapp-Sidik-Jonkman random effects meta-analyses of randomised control trials (RCTs) in inter-professional bidirectional collaboration between GP and pharmacists assessing a change of patient cardiovascular risk in the primary care setting.
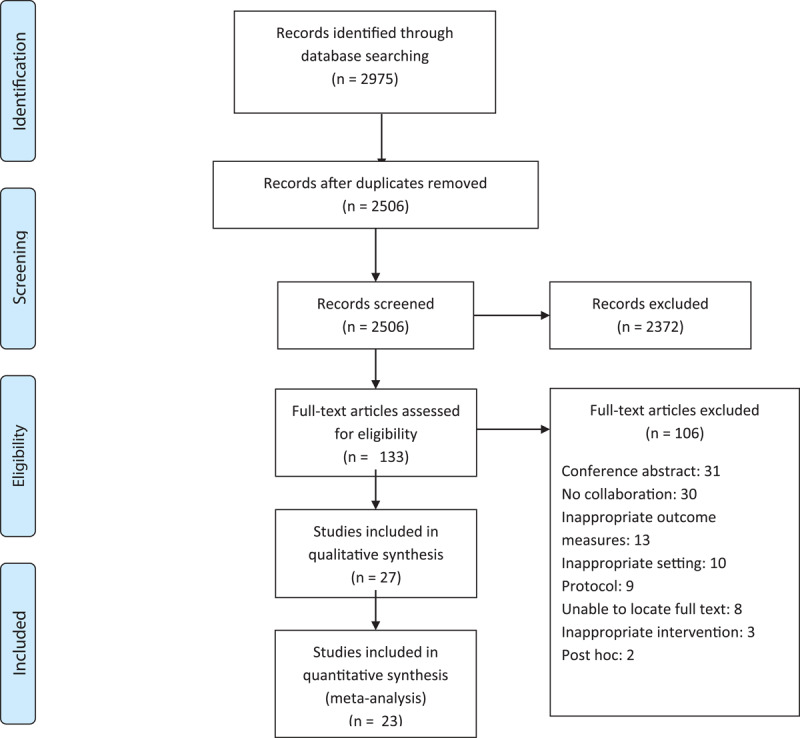
Data sources: MEDLINE, EMBASE, Cochrane, CINAHL and International Pharmaceutical Abstracts, scanned reference lists of relevant studies, hand searched key journals and key papers until August 2021.
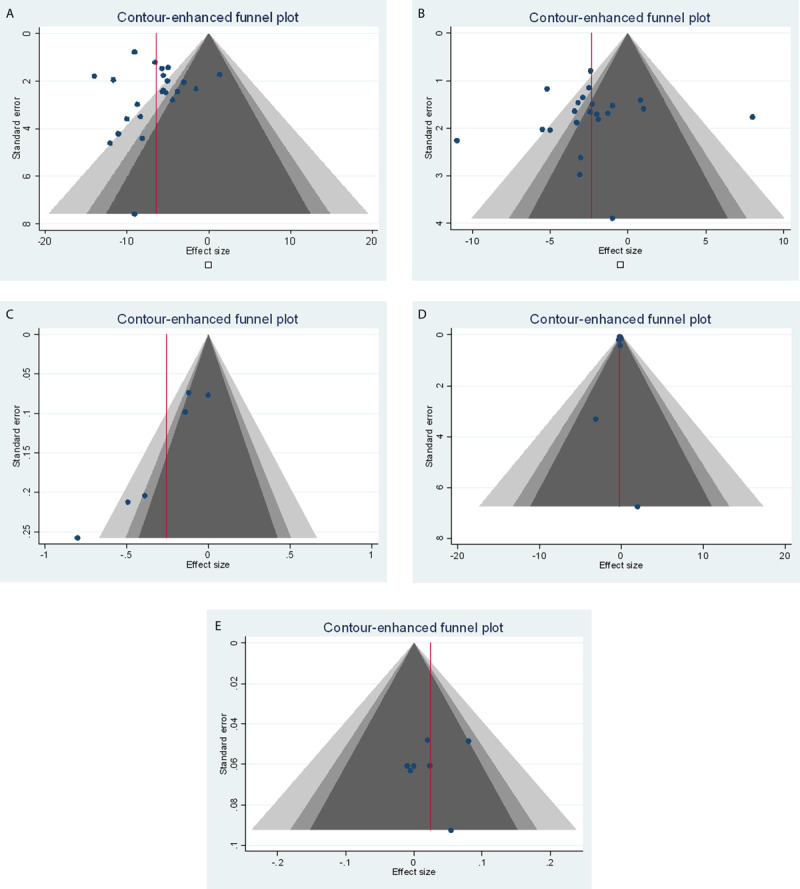
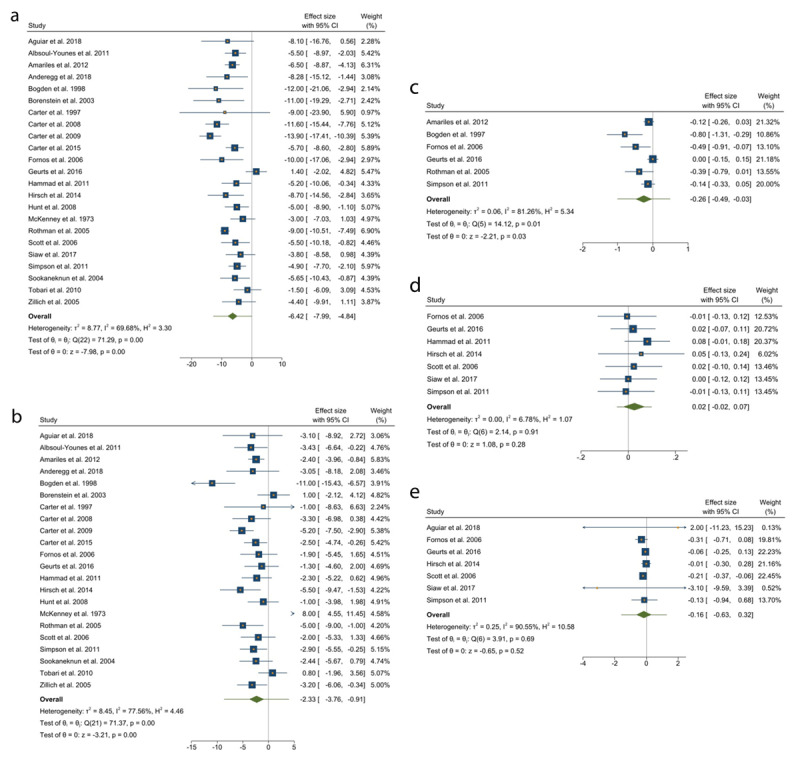
Data synthesis: Twenty-eight RCTs were identified. Collaboration was associated with significant reductions in systolic and diastolic blood pressure (23 studies, 5,620 participants) of -6.42 mmHg (95% confidence interval (95%CI) -7.99 to -4.84) and -2.33 mmHg (95%CI -3.76 to -0.91), respectively. Changes in other cardiovascular risk factors included total cholesterol (6 studies, 1,917 participants) -0.26 mmol/L (95%CI -0.49 to -0.03); low-density lipoprotein (8 studies, 1,817 participants) -0.16 mmol/L (95%CI -0.63 to 0.32); high-density lipoprotein (7 studies, 1,525 participants) 0.02 mmol/L (95%CI -0.02 to 0.07). Reduction in haemoglobin A1c (HbA1C) (10 studies, 2,025 participants), body mass index (8 studies, 1,708 participants) and smoking cessation (1 study, 132 participants) was observed with GP-pharmacist collaboration. Meta-analysis was not conducted for these changes. Various models of collaborative care included verbal communication (via phone calls or face to face), and written communication (emails, letters). We found that co-location was associated with positive changes in cardiovascular risk factors.
Conclusion: Although it is clear that collaborative care is ideal compared to usual care, greater details in the description of the collaborative model of care in studies is required for a core comprehensive evaluation of the different models of collaboration.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


